Dental caries is a disease in which enamel and dentin are gradually eroded, due to the elimination of minerals by acid excreted from bacteria in tooth surface plaque. Dental caries is a chronic disease that occurs frequently. Once the tooth is destroyed by dental caries, the tissue does not regenerate. Unless the disease is detected and treated during the early stage, it continuously progresses, and causes acute serous pulpitis or acute purulent pulpitis, accompanied by severe pain. In extreme cases, it may cause osteomyelitis. As a result, neglected teeth with caries are extracted, and chewing and the aesthetic function are lost. Most oral diseases can be predicted to occur. In particular, dental caries can be prevented. According to the 2009 Health Insurance Review Statistics Index of the Health Insurance Review and Assessment Service [1], dental diseases occupy 3 of the top 10 diseases for which health insurance benefits are used. Pulpitis and periapical disease ranks first, gingivitis and periodontal disease rank third, and dental caries ranks fifth. Because pulpitis and periapical disease are caused by dental caries, total health insurance benefits for diseases related to dental caries were $ 638 million in 2009. This accounts for approximately 30% of total health insurance benefits, which tend to increase annually. Dental prosthetics placed after pulpitis treatment consumes the most cost among dental treatments; thus, it was excluded from health insurance. More than $100 billion is estimated to be spent on dental caries. Dental caries progresses to various dental diseases, and affects quality of life, such as the need for false teeth in the elderly. Eventually, dental caries increases health expenses, which may cause enormous economic and financial loss to the nation [2]. Advanced caries causes chronic pulpitis or pulp necrosis, and may cause an abscess or cystoma in the alveolar bone, with associated pain. However, dental caries is often considered less serious than systemic disease. Dentists mostly focus on treatment that generates a large income, rather than prevention or early diagnosis of dental caries [3]. Generally, dental caries progresses during the demineralization and remineralization process; minerals are removed from the tooth surface during the former, whereas they are deposited during the latter. If the balance is broken by bacteria-secreted acids, demineralization occurs more frequently, which causes dental caries. Thus, many studies have been performed to remineralize teeth using appropriate prevention, such as fluorine applications during the early stage of the demineralization process [4].
Dentists have used pictures, probes, and X-rays to detect caries incidentally. As technology has developed, the accuracy of incidental caries detection has improved, particularly at the early stage. The previous method could detect caries only if one-third to one-half of the enamel was demineralized. In particular, Xrays frequently used in clinics show demineralized sites as normal tissue before the minerals have dissolved more than 40% of the tooth. Thus, removal of caries that create cavities and fillings are treatments that can be performed for this condition. Therefore, it is most important to diagnose dental caries in the early stage, to restore teeth to their original state using a non-invasive method. Recently, studies have been performed for the early diagnosis of dental caries, and drug treatment from surgical repair by creating cavities [5]. Therefore, studies on accurately diagnosing caries during the early stage are necessary.
The final objective of a dental caries diagnosis is to determine the necessity for treatment. Thus, it is very important to develop new technologies aimed at identifying caries lesions, to reduce unnecessary treatment. X-rays used for diagnosis carry a risk of radioactivity, as well as difficulty in diagnosing caries during the early stages. Thus, more accurate equipment is necessary to diagnose caries during the early stage. It is essential to identify a way to diagnose initial caries when white lesions or cavities have not yet occurred. Digital imaging fiber optic trans-illumination (DIFOTI) is a diagnostic method in which a light source with a range of high transmittance wavelengths penetrates the teeth from behind. DIFOTI is performed to observe the inside of teeth,
particularly for diagnosing incipient dental caries [6]. Currently, it is relatively adequate for detecting incipient dental caries; however, the subjectivity of the information obtained during light penetration into the teeth is a problem. Even though it is widely commercialized, clinical evidence has not yet been reported.
The quantitative laser/light fluorescence (QLF) system has similar problems. Fluorescent images are obtained from ultraviolet rays. The fluorescence occurring from QLF is in the yellowish green region. In this range, demineralization can be evaluated as deep using absorption and the yellow caused during demineralization. Diagnodent detects infra-red light fluorescence using a 655 nm diode laser that measures fluorescence in the demineralized area caused by deposited organic matter. Thus, its sensitivity and specificity are not appropriate for detecting incipient caries.
Most imaging methods based on the optical characteristics of teeth are considered as the best diagnostic methods. Unlike radiation, the optical method is hygienic, and not harmful to the patient’s health. In addition, two- or three-dimensional information can be acquired in real-time.
This study aimed to overcome the limitations of existing methods, by identifying tooth scattering characteristics. Specifically, long wavelength high transmittance infrared light was irradiated onto the enamel layer from the front, to provide highly accurate diagnoses of incipient caries. This study focused on the fact that the enamel layer has high transmittance in the range of infrared light, but strong scattering is caused by the heterogeneous structure after demineralization. Thus, we used a light-emitting diode (LED) with high brightness and various wavelengths as a light source. An imaging acquisition program was employed, to offer two- and three-dimensional image information on the teeth. The DIFOTI and QLF systems were employed and compared with diagnodent pen 2190 (Kavo, Germany), to determine whether incipient caries can be detected using a front-illuminated infrared light scattering image.
2. METHOD OF SKIN REGION DETECTION
Twenty healthy premolar teeth extracted for orthodontic treatment in private hospitals or clinics, or suspected to be under an incipient demineralization condition without cavities, were washed in running water, cleansed three times consecutively for 5 minutes in an ultrasonic cleaner, and stored in the freezer.
2.2 Implementation of the DIFOTI system
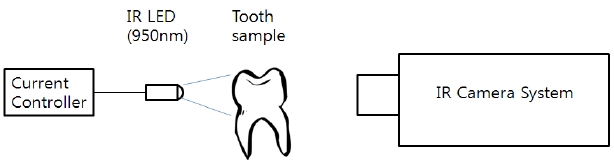
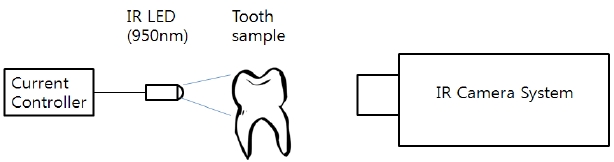
Images transmitted from the rear of the teeth using an infrared light (950 nm) source were observed. Because infrared light images cannot be obtained using an infrared light filter with a general camera, an infrared camera system was used (Fig. 1).
2.3 Implementation of the QLF system
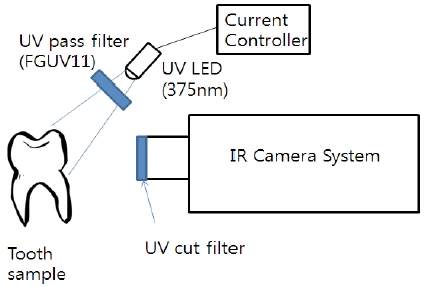
Images transmitted from the front of teeth using ultraviolet
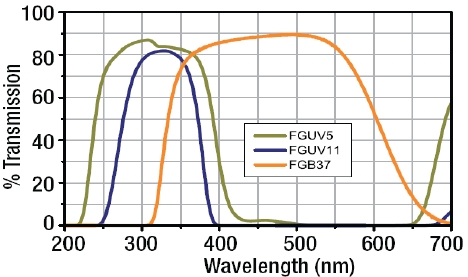
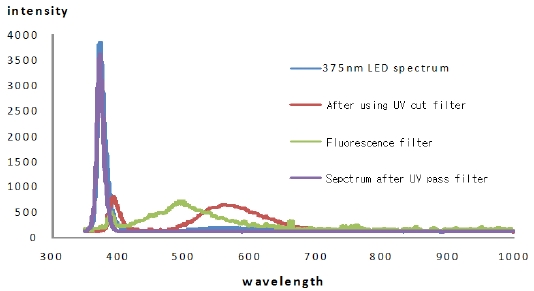
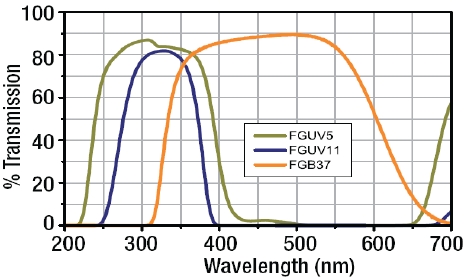
rays (375 nm) and an LED light source were observed. The results showed that the LED affected the fluorescence images, since LEDs emit light in the range of 500-600 nm. Thus, the LED was illuminated from the front using a UV-passing filter (FGUV11 - Ø25 mm UG1 Colored Glass) (Fig. 2).
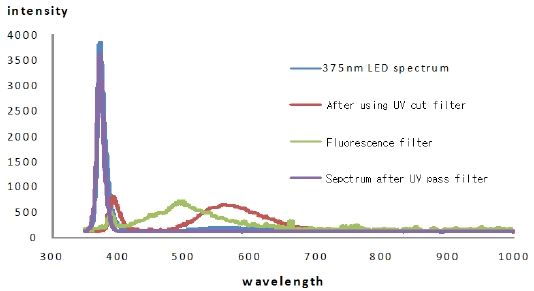
Figure 3 shows the spectral changes after using the UV-passing filter.
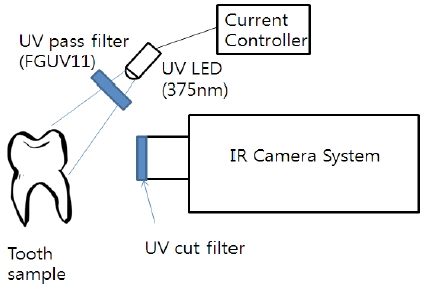
A diagram outlining the implementation of the QLF system in the laboratory is shown in Fig. 4.
2.4 Laser fluorescence device (LFD)
Laser fluorescence devices (LFDs) are widely used as a method to identify caries, and have recently become commercially available. LFDs show fluorescence in the range of 700-800 nm, which occurs in caries lesions from 0 to 99, using a 655 nm laser light source with signal sound.
2.5 Design of front-illuminated infrared light scattering
To diagnose demineralized caries, infrared light with little scattering should be used for investigating the enamel layer. In particular, if scattering of the enamel layer is weak, a clearer
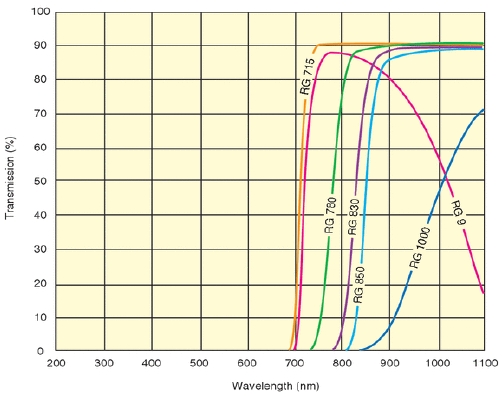
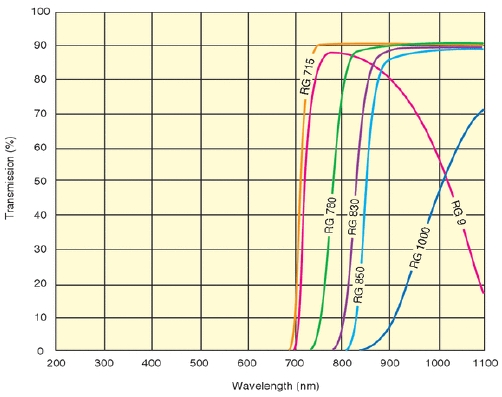
contrast can be obtained. Scattering images were obtained by illuminating the front of the teeth with a 950 nm LED. 950 nm light is not visible to the naked eye, but it can be observed using an infrared light filter under general light. Furthermore, scattering of infrared light can be observed using a light source that includes an infrared source, such as an incandescent bulb. The characteristics of the infrared light filter used in the experiment are shown in Fig. 5. RG 850 was used for the 950 nm LED.
Twenty sample teeth were examined in this study, and images of both the proximal and distal surfaces of each tooth were obtained using general light. The light sources from the DIFOTI and QLF systems were then illuminated. Forty images of teeth surfaces were obtained using each method, and 34 images were analyzed using the image-processing program developed in this study, excluding 6 tooth surfaces in which a demineralized region was not observed.
2.7 Estimation using diagnodent pen 2190
According to the user manual, diagnodent pen was adjusted so that the initial screen was 0. Without providing pressure, the fixed maximum value that appeared on the screen was considered the peak value of the tooth. Because reproducibility was low, the value was measured three times, and the average was selected as a representative value.
The image-processing program developed in this study was used to diagnose caries from sample teeth using DIFOTI images, QLF images, and front-illuminated infrared scattering images.
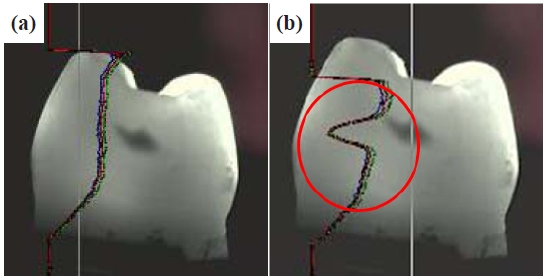
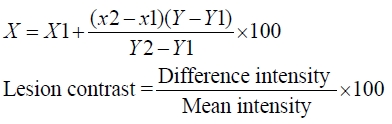
The RGB distribution was identified in the caries area diagnosed with sound area on the Y-axis in Fig. 6(a), and was saved as text. A curve-fitting method was used for the RGB values of the sound area in Fig. 6(b), and the peak value of the demineralized area was subtracted in equation 1. Lesion contrast of the sound area was then estimated using the Excel program with equation 2.
The diagnodent value of the same site was measured three times repeatedly, and the average was taken. SPSS version 17.K was used to analyze the results (SPSS, Inc., Chicago, IL, USA), and a simple linear regression analysis was performed for each method.
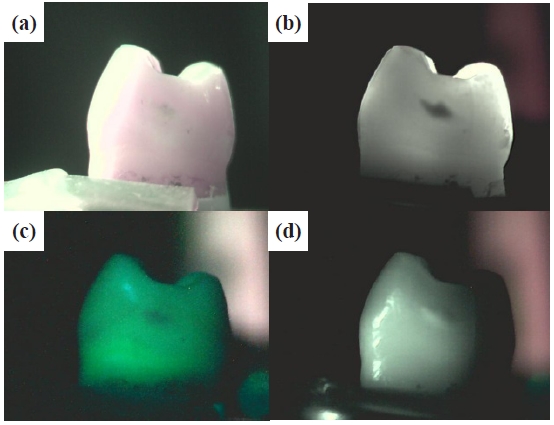
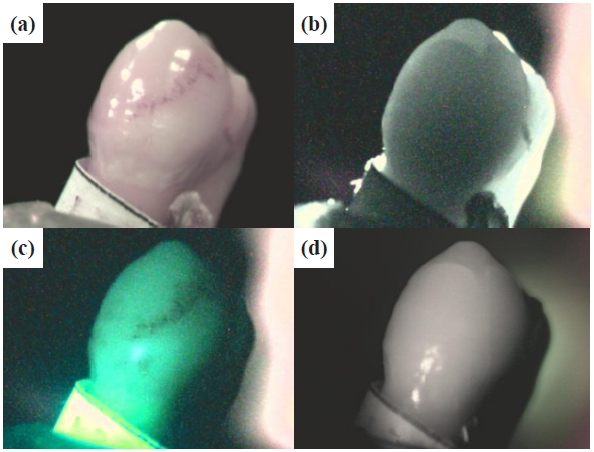
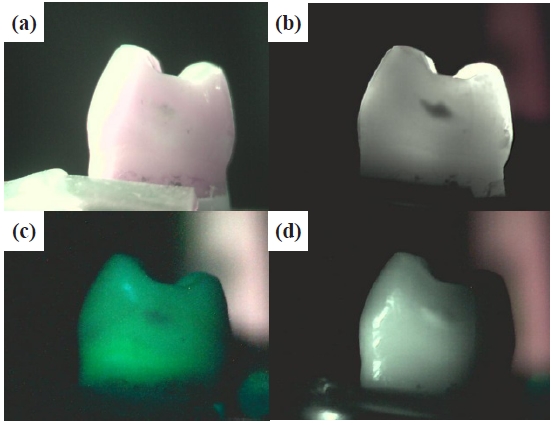
Images of the proximal and distal surfaces of the 20 sample teeth were examined, and incipient caries were identified under normal light, and on DIFOTI images, QLF images, and frontilluminated infrared light images (Fig. 7).
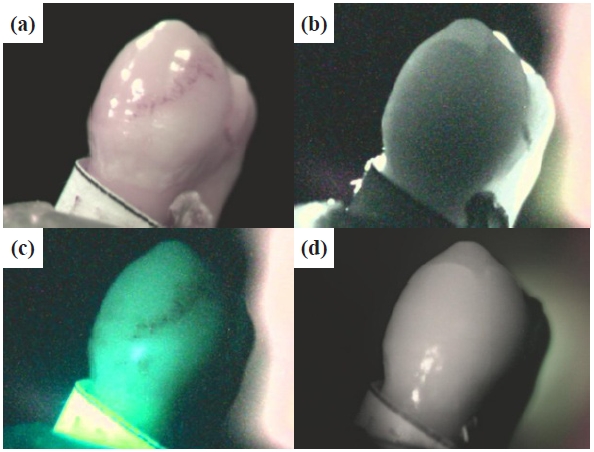
The front-illuminated infrared light method may not have provided appropriate illumination for the desired tooth surface; however, the lesion area was easily observed by illumination with the proper intensity of light, and the result was the same as that of DIFOTI. However, DIFOTI requires strong light when passing through thick areas of the teeth and it was difficult to obtain appropriate light. In particular, teeth that turned yellow without caries were identified under normal light (Fig. 8).
DIFOTI images and front-illuminated infrared light images did not show caries. In contrast, QLF produced images that could be used to identify caries, as the colored or dirty area was black. The front-illuminated infrared light method produces scattering, due to heterogeneous structures such as hard tooth tissue; however, scattering is rare in the enamel layer, and absorption does not occur for the colored area of organic matter.
A relatively high level of scattering occurs in dentine. If the light was illuminated vertically from the front, it was difficult to observe sufficient scattering. Thus, an excellent image was obtained if the light passed through the enamel layer only.
3.2 Regression analysis of lesion contrast values for each tooth by tooth surface
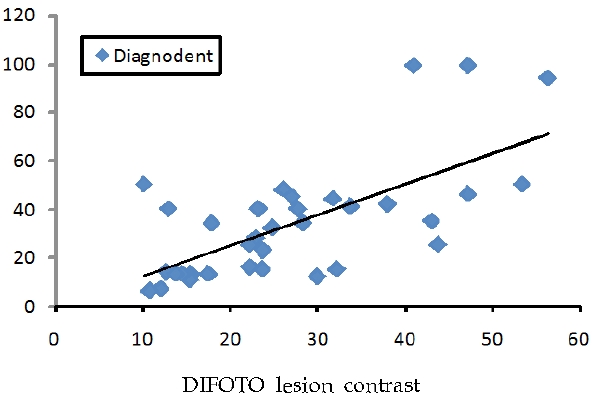
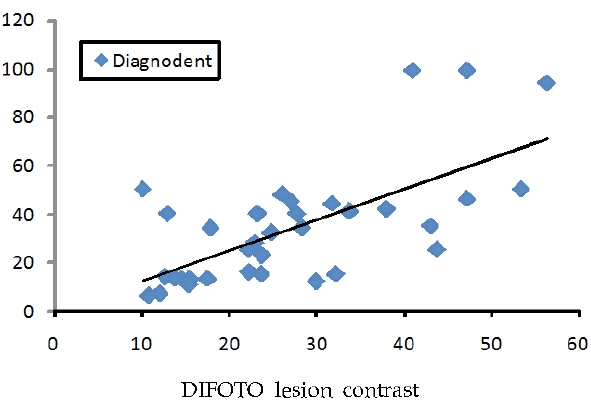
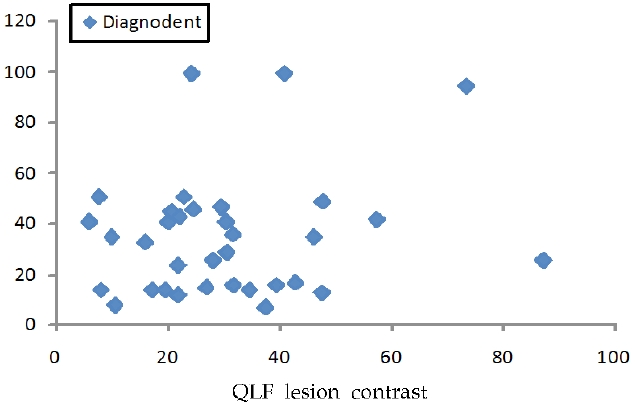
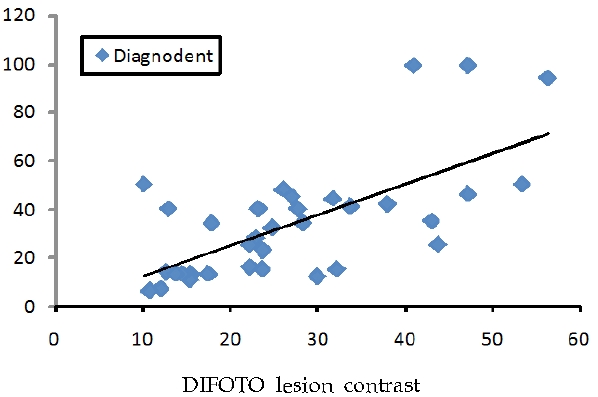
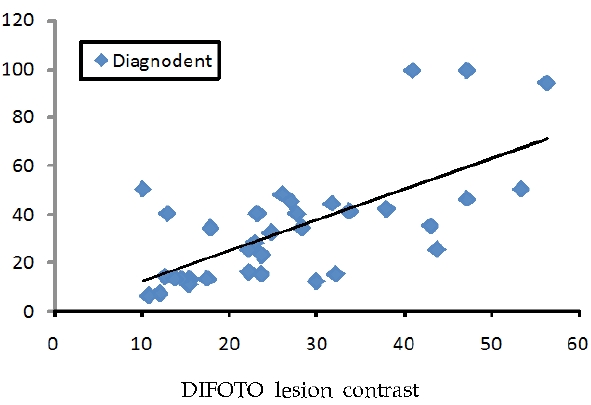
Linear regression analysis showed a significant correlation between DIFOTI images, QLF images, forward IR images, and diagnodent values (r = 0.67 for diagnodent value on DIFOTI lesion contrast; p < 0.01; Fig. 9).
For DIFOTI lesion contrast versus forward IR scattering lesion contrast, the r value was 0.35, which indicates a significant in-
crease (p < 0.05, Fig. 10).
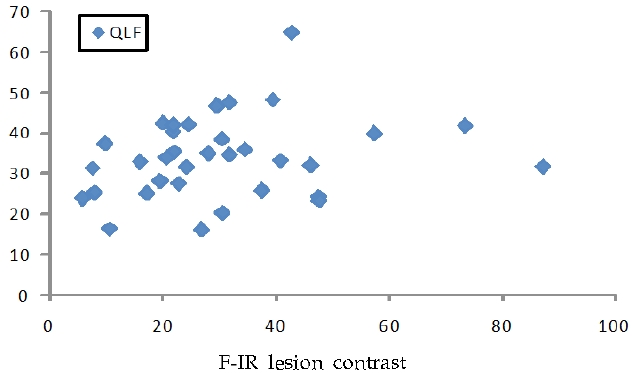
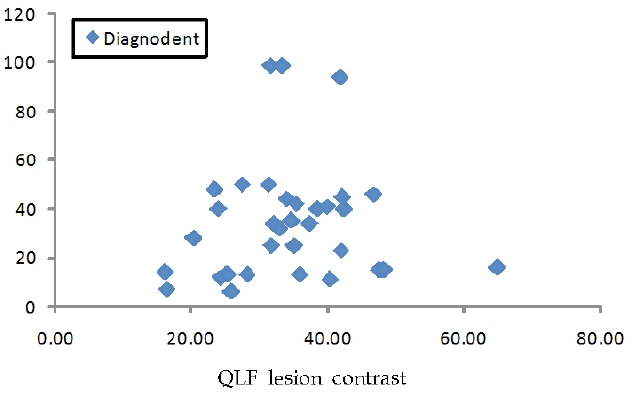
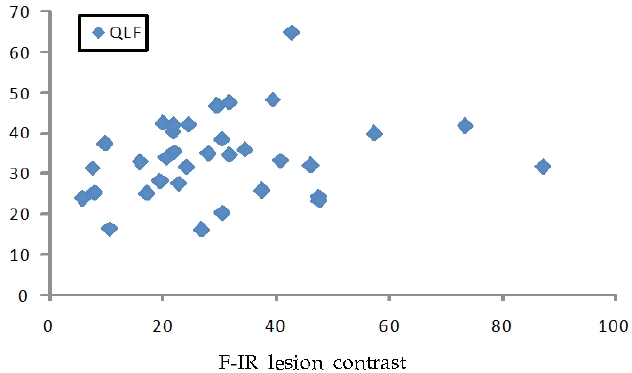
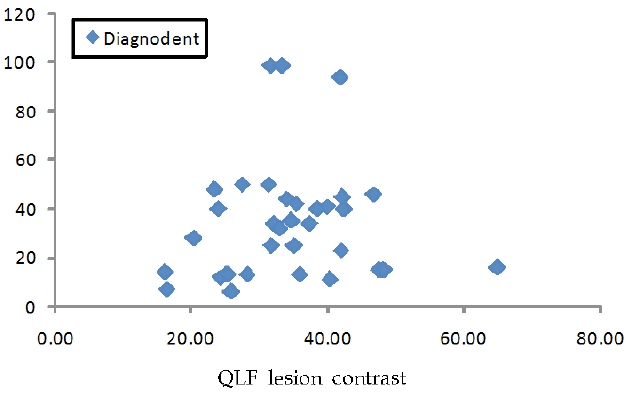
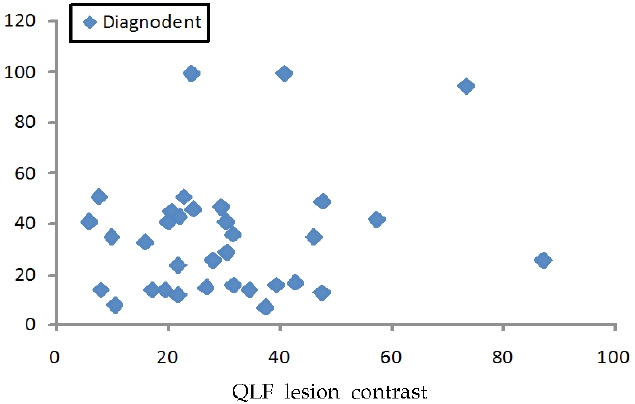
However, no significant differences in the QLF lesion contrast versus forward IF scattering lesion contrast (Fig. 11), or the diagnodent value versus the QLF lesion contrast, were observed (Fig. 12). Further, no significant difference between diagnodent values versus the forward IR lesion contrast was observed (Fig. 13).
Dental tissues destroyed by dental carries are not regenerated. However, during the early stage of dental caries, demineralization and remineralization occur at the same time under a normal oral cavity environment [7]. Even before a cavity forms, demineralization should be detected, and the current status should be diagnosed to prevent the formation of a cavity.
The objective of early diagnosis is to remineralize enamel, using a non-invasive method. Therefore, it is most important to develop an accurate and highly sensitive diagnostic method that detects incipient enamel caries [8].
Bjelkhagen et al. [9] first reported that fluorescence decreases in demineralized enamel. Since then, many studies on the fluorescence characteristics of teeth [10], characteristics of ultraviolet fluorescence [11], and argon laser light characteristics have been conducted [12]. Thus, QLF has relatively high diagnostic ability for incipient caries on smooth and occlusal surfaces.
The DIFOTI system was improved from the fiber optic transillumination (FOTI) system, which uses differences in light transmission between normal and abnormal tissues. FOTI uses an analog camera and image storage device, to save and manage images on a computer [13]. It shows excellent diagnostic abil-
ity, as compared with existing bite-wing radiograph images of proximal caries. Hwang [14] suggested that the DIFOTI system shows a significant reverse correlation with the depth of lesions measured by confocal laser scanning microscopy as the gold standard, and is able to accurately measure the level of smooth demineralization and remineralization. However, the light source volume is large, and the light generates significant heat. Recently, Lee et al. [15] studied a new LED light source system to solve the problem of high heat and large volume. In an in vitro experiment, caries enamel transmission between the existing DIFOTI system and the prototype DIFOTI system decreased significantly.
Among existing caries diagnostic tools, optical imaging diagnostic systems that are non-invasive and real-time are preferred. Optical imaging diagnostic systems have many desirable characteristics. For example, these systems do not have invasive or sanitary problems, such as with palpation, and they use safe electronic waves, unlike X-rays. Nevertheless, they are very expensive, because the imaging acquisition analysis systems and light source costs are very high.
Recently, a multimedia concept was introduced to computer, mobile phone, and camera systems that acquire and store video. The capacity has been improved and the price has become economical. In addition, LEDs can be used that produce ultraviolet light, which was previously difficult to obtain, and infrared light with a very long wavelength. Thus, the present study implemented image processing using this system, and investigated diagnostic methods for incipient caries. The LED light source for the experiment varied from 375 nm UV light to 950 nm infrared light. Wavelength was measured using a spectrometer (Ocean Optics, SpectraSuite software, Dunedin, FL USA). Light source images by wavelength were acquired with a digital camera system. Siliconbased CMOS and CCD sensors were used to detect the range of infrared light. The caries imaging program developed in this study was used to perform the image analysis.
The results of reflection and transmission images measured by wavelength indicated that the caries clearly showed fluorescence, but transmitted light was not observed accurately in the red area. In addition, the incipient caries area was not observed in the range of forward-illuminated visible light wavelengths. Colored or discolored areas were not visible from the infrared transmitted image, but blue and ultraviolet fluorescence images were more than satisfactory. Therefore, an excellent diagnosis is possible, if sensitive light sources are used in combination to distinguish various lesions.
Studies on various wavelength ranges indicate that demineralization is clearly shown with forward-illuminated infrared, unlike with visible light illumination. This result mean that sattering in the demineralized area markedly increased rather than scattering in enamel layer was very light under IR, such as sanding and smoothing the surface of translucent glass with sandpaper.
In this study, LEDs with various wavelengths were used as the light source, and an image-processing program was implemented to offer two- and three-dimensional dental images. Furthermore, the DIFOTI and QLF systems were implemented and compared. These systems were also compared with the diagnodent pen 2190, to investigate the possibility of an incipient caries diagnosis using forward-illuminated IF scattering images.
Through image analysis using the three systems, two proximal and distal surface areas were measured from 20 sample teeth, and 40 images were acquired. Six dental surfaces in which no caries occurred were excluded from the analysis. Similarly, a diagnodent value was identified in the same area. To compare forward-illuminated infrared scattering, an RGB distribution curve was used on the same caries area from images obtained using each method. DIFOTI images were the best, and forwardilluminated IR scattering showed excellent caries diagnostic ability. However, by comparing differences in optical density in the normal and caries area, a method to measure demineralization can only be suggested. The regression analysis results for each method indicated that the diagnodent value versus DIFOTI lesion contrast was statistically significant: r = 0.67 (p < 0.01), and that the DIFOTI lesion contrast versus forward-illuminated IR scattering lesion contrast increased significantly (r = 0.35; p = 0.056).
However, no statistical significance was found for the QLF lesion contrast versus the FIR lesion contrast, or the diagnodent value versus the QLF lesion contrast. In addition, no significant difference was found between the diagnodent value and FIR lesion contrast.
QLF and diagnodent are fluorescence images generated by organic matter in teeth. For QLF, fluorescence in the range of 400 to 600 nm is absorbed by the coloration of the caries; therefore, it does not show structural information of demineralization alone. diagnodent indicates the area where demineralization was generated, but also does not measure the level of demineralization alone. Thus, FIR was correlated with the caries area diagnostic result from the DIFOTI method, which showed excellent images. There was almost no scattering in the enamel layer, and no absorption in the organic matter coloration area; scattering only occurred due to the hard structure of the teeth. diagnodent showed different results, based on the level and type of organic matter deposited in the caries area. In contrast, FIR is more accurate for incipient caries diagnosis, as it diagnoses structural dental disorders directly. Moreover, FIR lesion contrast is different from that of QLF, because it cannot measure the change in dental structure by demineralization, due to the influence of teeth coloration. The FIR method was similar to the DIFOTI method in terms of principle, and corresponding results were expected. In this study, surface reflection was not considered forward illumination; therefore, no significant difference in lesion contrast was observed between DIFOTI and FIR scattering imaging.
Incipient caries demineralizes approximately 300 μm to < 500 μm of the enamel layer, which is recovered through remineralization. If the recovery period is missed, permanent, irreversible dental damage occurs. Therefore, it is necessary to identify and treat the condition as early as possible. Many methods can be used to diagnose incipient caries. However, excellent methods such as QLF or DIFOTI diagnostic systems are very expensive, and there are limitations on the accuracy of detection of incipient carries. The enamel layer has a very low scattering rate in the range of infrared light, whereas the enamel demineralization area from incipient carries has a relatively high scattering rate, proportional to the level of demineralization. Therefore, when infrared light was illuminated onto the tooth, the light was transmitted into the enamel, and reflected to the demineralization area, where it was scattered in proportion to the level of carries. Scattering IR images were acquired by FIR. Contrast analysis with the adjacent area was used for incipient caries diagnosis, by quantitatively estimating the level of demineralization.
Lesion contrast of sound tissue was estimated for all images, to assure subjectivity. Regression analyses were performed on each method, and a significant correlation was observed for the diagnodent value versus the DIFOTI lesion contrast (r = 0.67; p < 0.01), and the DIFOTI lesion contrast versus FIR scattering lesion contrast increased significantly (r = 0.35; p < 0.05). However, no statistical difference was found for the QLF lesion contrast versus the FIR lesion contrast, or the diagnodent value versus the QLF lesion contrast. Similarly, no significant difference was observed between the diagnodent value and FIR lesion contrast. Thus, FIR results were correlated with diagnostic results, using the DIFOTI method. No scattering or absorption in the organic matter coloration area of the enamel layer was observed. Thus, only scattering by the hard dental tissue occurred, and excellent images were obtained.