In Kenya, traditional knowledge on herbal medicine has remained a mainstream source of maintaining wellbeing for generations in many communities. However, the knowledge has been eroded in the course of time due to sociocultural dynamics virtually advanced by Christianity and formal education especially in the Kikuyu community. The study documented current ethnobotanical knowledge and threat to the traditional knowledge on medicinal plants among the Kikuyu community. A survey was carried out in Mathira, Tetu, Kieni, Othaya, Mukurweini, and Nyeri Town constituencies. Thirty practicing herbalists were purposively sampled; 5 per constituency. Data was obtained through semi - structured questionnaires and analyzed both qualitatively and quantitatively. A total of 80 ailments treated using 111 medicinal plant species distributed within 98 genera and 56 families were documented. Prevalent communicable diseases treated using herbal medicine included; gonorrhea (17.5%), malaria (15%), respiratory infections (12%), colds (10%) and amoebiasis (10%). Non-communicable diseases were; joint pains (11.1%), ulcers/hyperacidity (8.7%), high blood pressure (8.7%), intestinal worms (11.1%) and arthritis/gout (10%). Frequently harvested plant materials were; roots, barks and leaves. The study concluded that, traditional medicine practitioners in Nyeri County possessed wide knowledge of herbal medicine but this knowledge was on the verge of disappearing as it was largely a preserve of the aged generation. The study recommended massive campaign about the benefits of using herbal medicine in the study area. Further pharmacological studies are recommended on the mentioned plant species aimed at establishing their efficacy and safety as well as standardization as potential drugs.
Traditional knowledge on herbal medicine has remained a mainstream source of maintaining wellbeing for generations in many communities (Kamboj, 2000). However, while many communities in Africa are custodian of sophisticated plant knowledge (Barrow, 1996), adoption of western culture has caused rapid erosion of indigenous knowledge (Fratkin, 1996). The Kikuyu community which largely occupies central Kenya had most of its culture eroded by western influence as a result of Christianity, colonialism and formal education (Sindiga et al., 1995). During the colonial period, Nyeri County witnessed unprecedented early missionary establishment notably, Tumutumu Mission in 1908. This was followed by establishment of a hospital, school and a church by the Scottish Mission. The mission was a spring board and focal point of Christianity and education establishment in other parts of Nyeri region (Presbyterian Church of East Africa, 2011). Similarly, the Catholic missions particularly, Consolata fathers established a mission in Nyeri in 1910. The mission established a primary school in 1924 which is today’s Nyeri High School and, several other schools. Consolata hospital was established in the same place in 1937 (Njoroge, 1999). To date, Nyeri County enjoys one of the highest literacy levels in Kenya (Kenya National Bureau of Statistics, 2013). The spread of Christianity and introduction of formal education brought about unprecedented changes (Sindiga et al., 1995). It came with a cost especially on the loss of traditions which the missionaries considered barbaric. Missionaries were disdainful of African traditional beliefs, attitudes and practices. They were guided by “counter cultural” model of Christian-culture interaction based on the assumption that Christianity and indigenous practices were diametrically opposed and the latter would have to give the way (Bevans, 1992). Particularly, use of traditional medicine faced a major setback due to alleged association with witchcraft and perceived potent of western medication. Consequently, use of traditional medicine among other cultural practices was condemned and prohibited among converts (Muraya, 2013). The effort of missionaries was boosted by colonial government which introduced the "Witchcraft Act" of 1925” outlawing traditional medicine in Kenya (Sleap, 2011). Moreover, establishment of hospitals alongside schools provided an alternative source of healthcare provision (Njoroge, 1999). From the foregoing, the Kikuyu culture within which knowledge on traditional medicine is engrained was rendered amorphous. Nonetheless, the post-independence era witnessed Kikuyu community from Nyeri County grapple with high prevalence of non-communicable diseases (http://integratepc.org/hospitals/kenya-only/) that defied conventional treatment approaches (Lucado et al., 2011). Further, high incidences of ailments which were resistant to antibiotics (Laxminarayan and Heymann (2012) continued to challenge allopathic mode of treatment. This may have driven the community to seek alternative treatment methods, notably, several herbal clinics were opened especially in urban centers in Nyeri, an indication that traditional medicine was gaining acceptance in Central Kenya. However, future ethno therapeutic studies of traditional medicine used by the Kikuyu community from Nyeri County relied on the preservation and protection from extinction, of traditional medicinal knowledge engrained in the pre-colonial Kikuyu cultural heritage. World Health Assembly (1987) expressed the need for member countries to develop programmes for conserving cultural medicinal knowledge (Eloff, 1998). This endeavor could only be achieved through detailed documentation of ethnobotanical knowledge of different communities. Njoroge and Bussmann (2006) and Bussmann and Njoroge (2007), documented herbal medicine for skin and, eye, ear and throat (ENT) around Mt. Kenya and commonly sold herbs around urban centers in central region of Kenya. Despite the reported rise in use of herbal health services in Kenya, little published data was available on traditional knowledge on herbal medicine used in Nyeri County. The purpose of the current survey was to investigate and document comprehensively, traditional medicinal plants used in the treatment and management of ailments in Nyeri County.
>
Study area and ethnographic background
Nyeri County occurs in Central Kenya and it borders; Laikipia County to the North, Nyandarua to the West, Murang’a to the South, Kirinyaga to the East, and Meru to the North East (Fig. 1). It is located between latitude 0.4167° S, 36.9500° E. At the time of the study, it had a population of 693,558 (Male – 49%, Female – 51%) occupying an area of about 3,337 km2. It is divided into six constituencies; Tetu, Othaya, Kieni, Mukurwe-ini, Mathira and Nyeri town. The temperature ranges from an average annual minimum of 12℃ to a maximum of 27℃ and receives rainfall amounts from 550 mm to 1,500 mm per annum. The long rains starts on March and ends on May while the short rains sets in from October to December. Nyeri County leads nationally with a forest cover of 38.5% as compared to a national cover of 6.99%. The major geographical landscapes of the County are Mount Kenya (5,199 m) and the Aberdare ranges (3,999 m) to the east and west, respectively; both are densely forested with rich plant species diversity. Agricultural activities are a source of livelihood and the most predominant economic activities include; tea and coffee which are grown for exports, large scale horticultural flower farming, greenhouse farming by small scale vegetable farmers and dairy farming. The most predominant tribe is the Kikuyu community; others included the Kamba, Luo, Meru, Embu, Somali, and Borana. Most of the people living in Nyeri County are of Christian faith. Nyeri County has one level 5 hospital, three level 4, 18 level 3 and 75 level two health facilities. It has three mission and three private hospitals, one hospice, one nursing home and 228 private clinics which are spread across the County. The doctor/population ratio is about 1:6459 and a nurse/population ratio is 1:143.
>
Study design and data collection
The study was a cross sectional survey, 30 practicing traditional medicine practitioners (TMPs) that willingly consented to participate were purposively sampled (5 per constituency), through the guidance of officers from Ministry of Culture and Social Services. The criteria for selecting the target population were guided by Cohen et al. (2000). According to the authors, a sample of 30 respondents is the minimum sample size that can reveal the full range or nearly full range of potentially important opinions when seeking qualitative data as well as in working out statistical analysis in quantitative data. Inclusion criteria were based on those TMPs that were born and practiced in the study area. Data collection involved interviews, administration of pilot tested semi-structured questionnaire to the TMPs, and transect walk. Interviews were conducted in the native language (Kikuyu) and translated to English by a team of trained research assistants. The respondents were assured of confidentiality and that, any information volunteered would be used for research purpose. Information collected from the TMPs included; demographic information, traditional knowledge on herbal medicine (harvesting, processing, dosage, preparation, route of administration and toxicity) and challenges in herbal medicine practice.
>
Sample collection and identification
Medicinal plants used to treat diseases that were mentioned by the TMPs during the interview were collected by a team of researchers from the University of Nairobi, research assistants and TMPs. The plants were identified by a botanist and voucher specimens were deposited at the University of Nairobi Herbarium. Information about; habit, habitat, plant part harvested and scientific name was recorded.
Both qualitative and quantitative data were collected during the study. Qualitative responses were organized into themes while others were presented verbatim. Quantitative data from demographic information as well as quantified qualitative data were presented as proportions, percentages, pie charts and bar graphs as well as analyzed using SPSS Version 20. The relevance of medicinal plant species among traditional medicine practitioners was calculated using the formulae; UVs (total Use Value of the species for all informants) = (ƩUVis) / (ni); UVis is the Use Value of the species for a single informant and nis is the number of interviews by the informant (Hoffman, 2007; Phillips and Gentry, 1993).
Majority of the Traditional Medicine Practitioners (TMPs) were over 57 years (87%) and were of Christian faith (89%). Seventy seven percent (77%) had formal education out of which 55.6% had undergone professional training and worked in the formal sector; however, 20% had since retired. Sixty seven percent (67%) combined herbal practice with other income generating activities such as; business, farming, masonry and formal employment, the other 33% of the practitioners earned their living from herbalism. The TMPs had long standing experience; 89% had practiced for over 20 years, the other 11% between 6-10 years. They mainly practiced from their homes (78%); the other 22% had established a clinic at either Karatina, Mweiga and Nyeri town. Additionally, they had acquired their skills in herbal medicine through inheritance from parents and long-standing experience. Notably, there was no evidence of apprenticeship or organized structures of passing down knowledge which they possessed. However, 67% had acquired additional information from books, media and internet. Fifty six percent (56%) had no formal training on herbal medicine while 44% had attended a government and World Bank sponsored seminar. The attendees displayed a deep mastery of appropriate herbal medicine practices during plant harvesting, preparation, storage, and dosage administration. They were aware of the group of patients that should be referred to medical practitioners for specialized treatment based on, age, sex and magnitude of sickness. Additionally, they learned management skills which included record keeping and financial management. Besides uplifting their confidence and self-esteem in the profession, the seminar had driven out fear among them. Eighty percent (80%) had registered as members of the Nyeri Herbalists Association (NYETIPA) under the Ministry of Culture and Social Services. A total of 80 ailments treated by TMPs were recorded, common communicable (infectious) diseases included; colds (53.3%), (50%), gonorrhea (40%), respiratory infections (33.3%), intestinal worms (33.3%), and amoebiasis (10.0%) while non-communicable diseases were; high blood pressure (43%), arthritis/gout (40%), wounds (40%), joint pain (33.3%), malaria ulcers/hyperacidity (33.3%), stomachache (33.3%), male sexual dysfunction (33.3%) and constipation/indigestion (33.3%). Some diseases were treated as one, like arthritis and gout and, ulcers and hyperacidity (Table 1). For the TMPs to achieve a wholesome effect they used a holistic treatment approach which included several herbs like; blood purifiers, appetizers, digestives and revitalizers and, nutritional vegetables such as stinging nettle and Macdonald’s eye. They combined 4-5 herbs in the treatment of one disease; some acknowledged using a cocktail of up to 20 herbs, thus the saying “
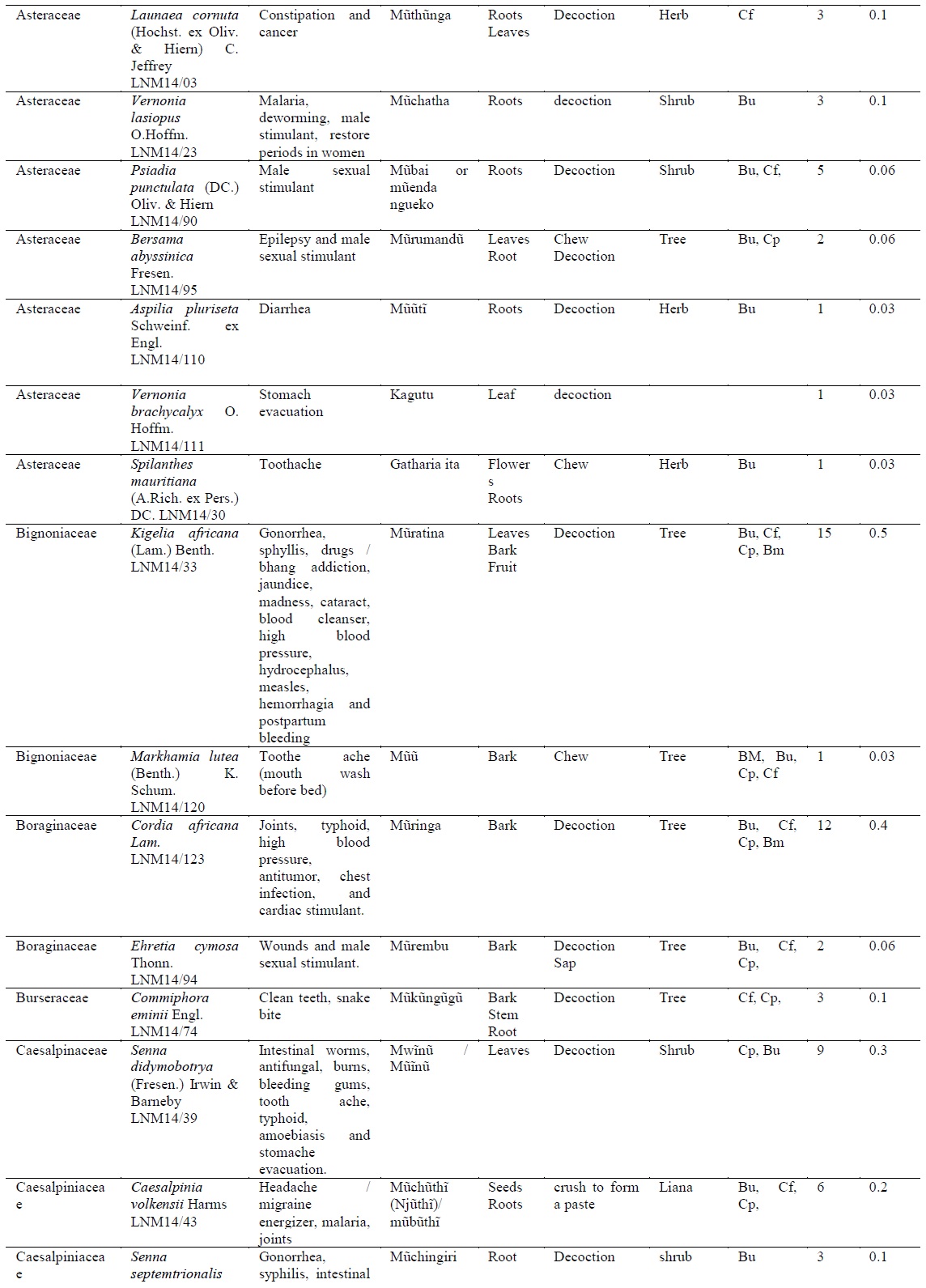
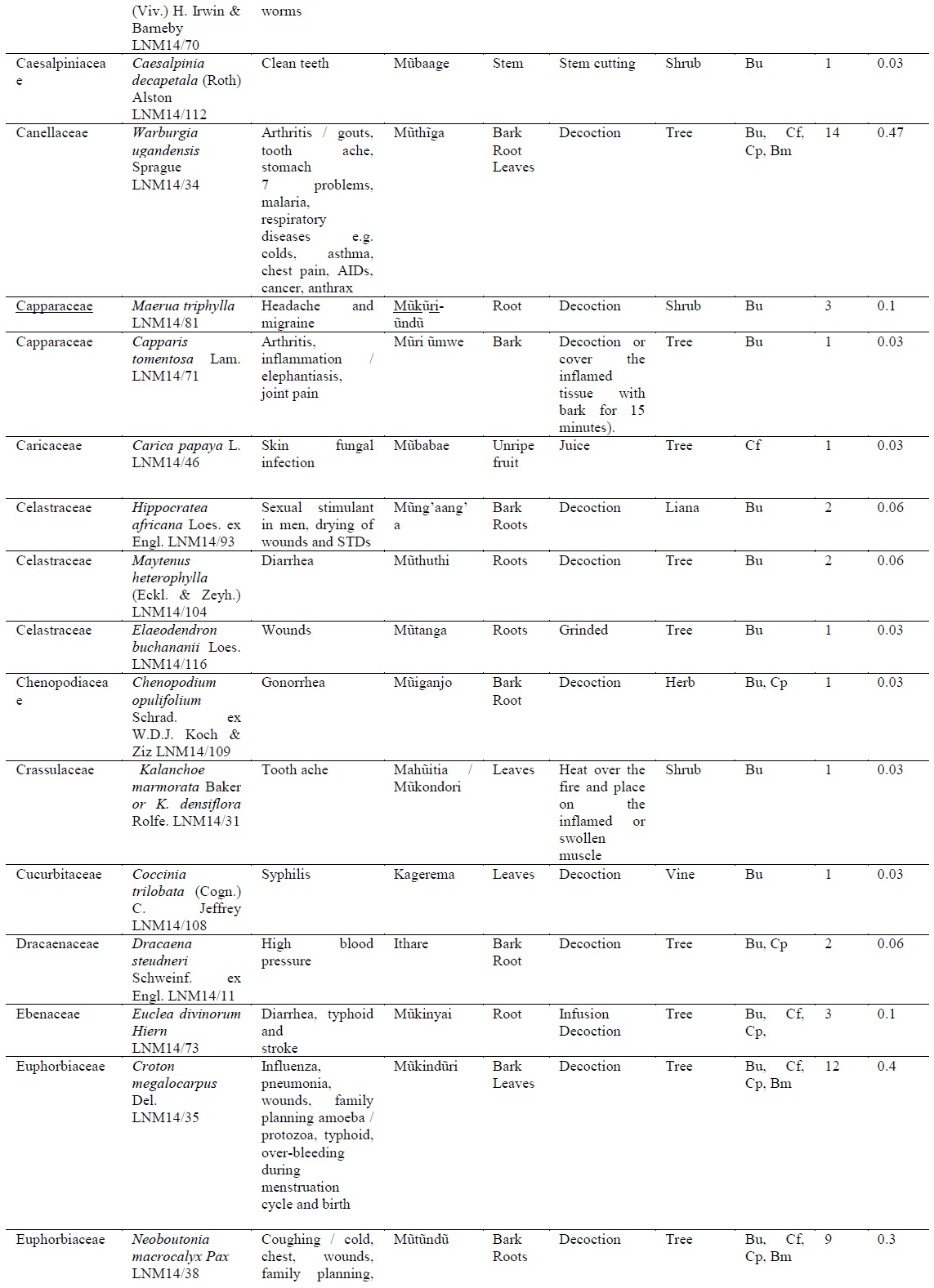
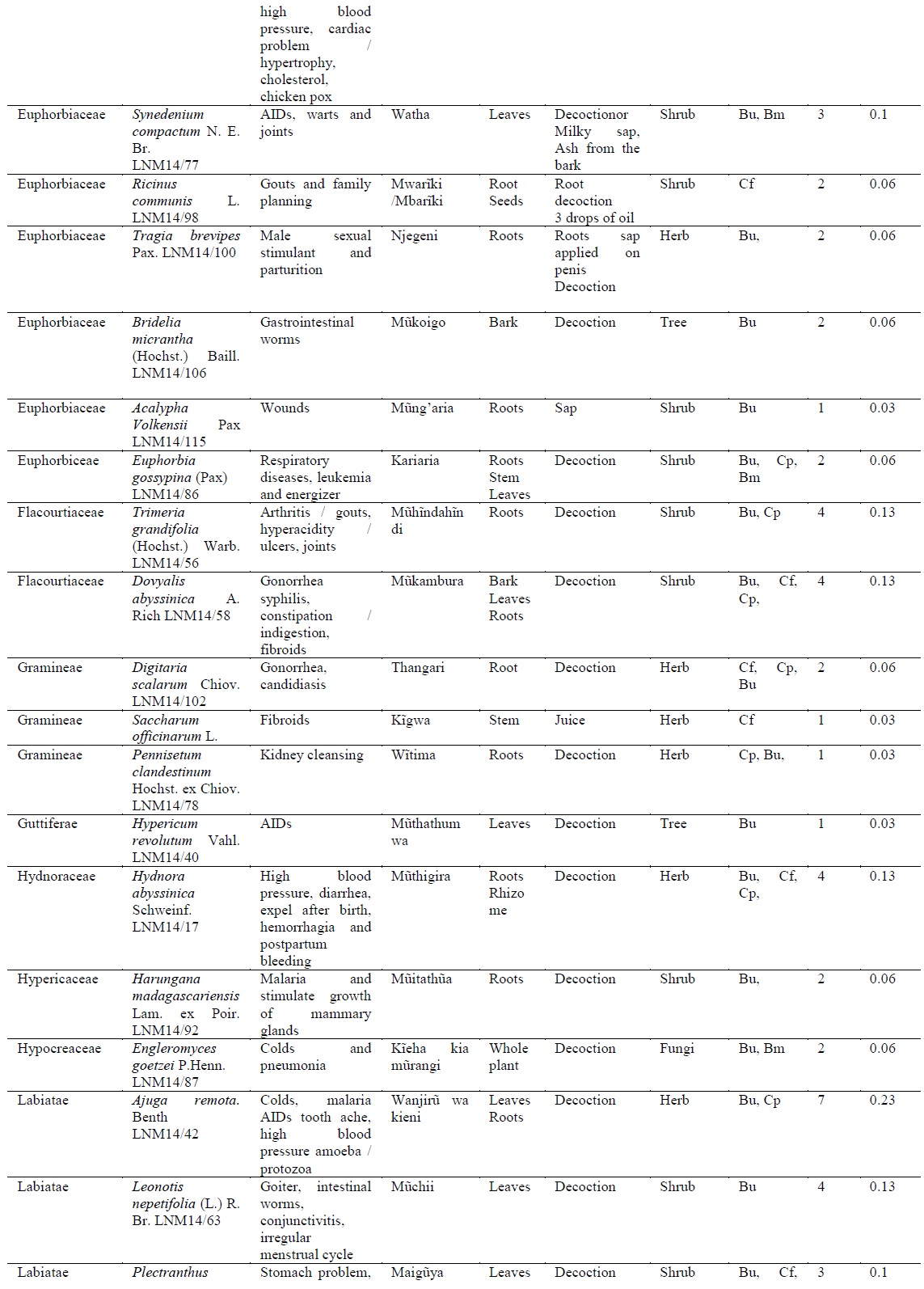
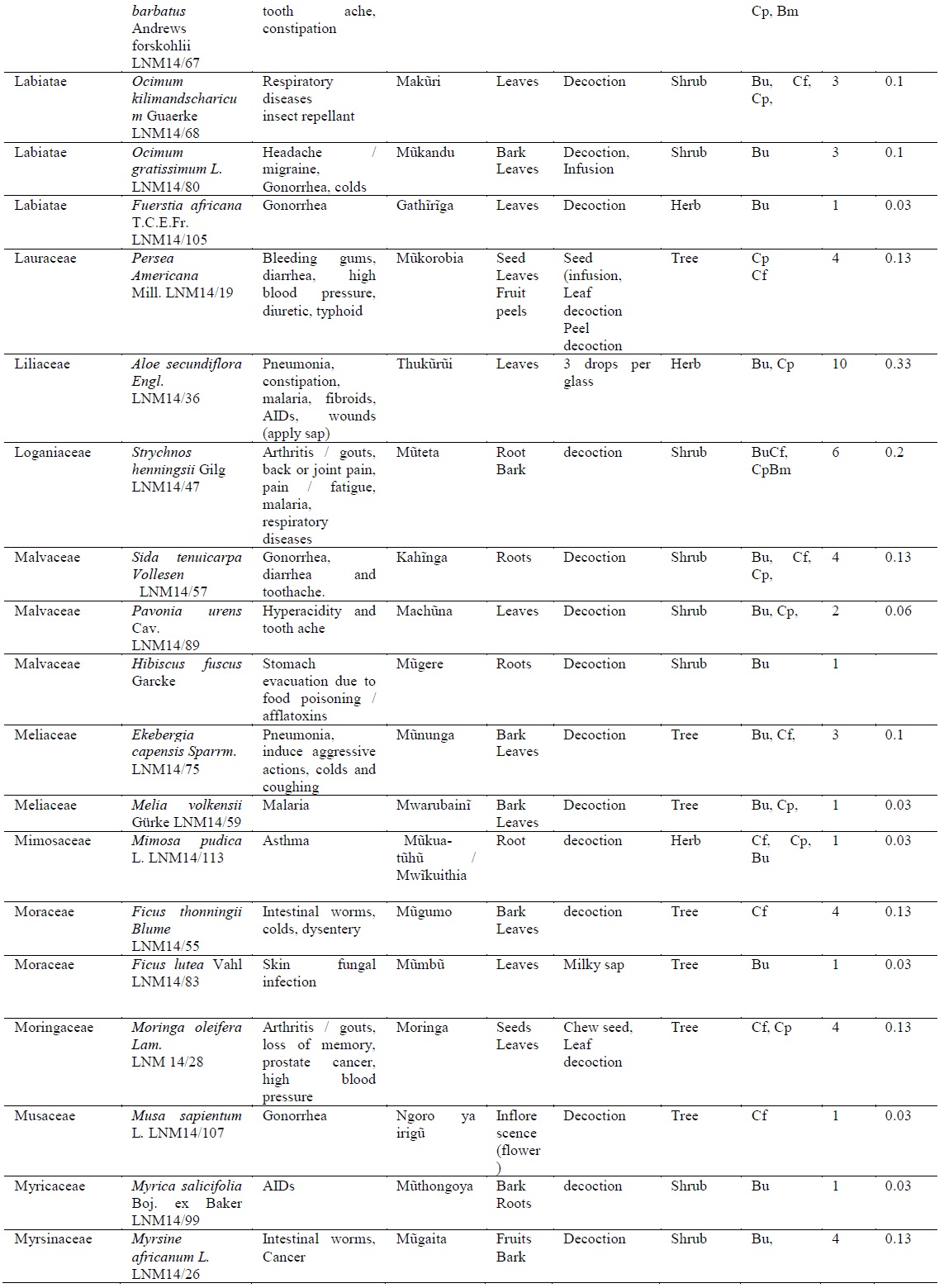
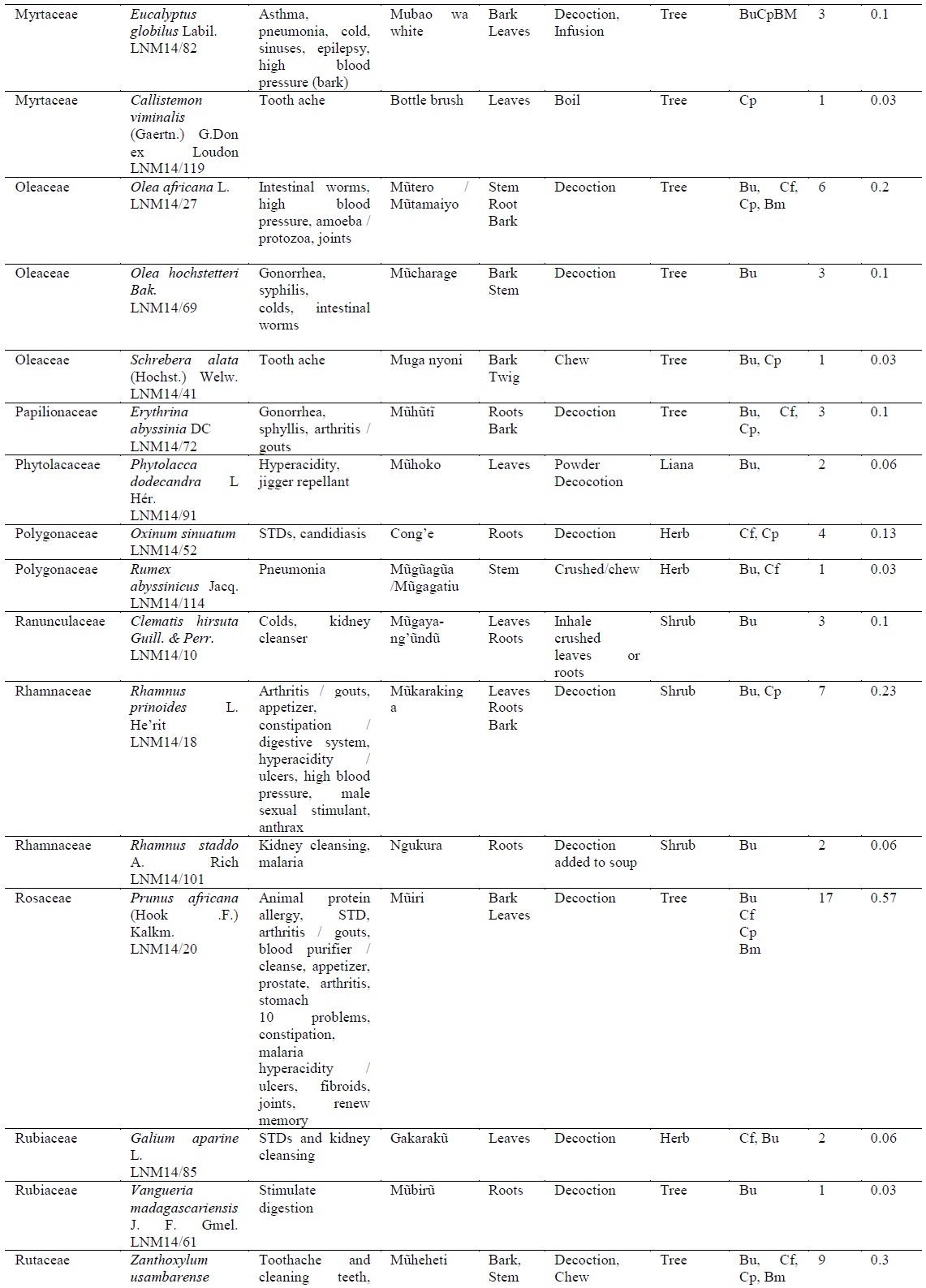
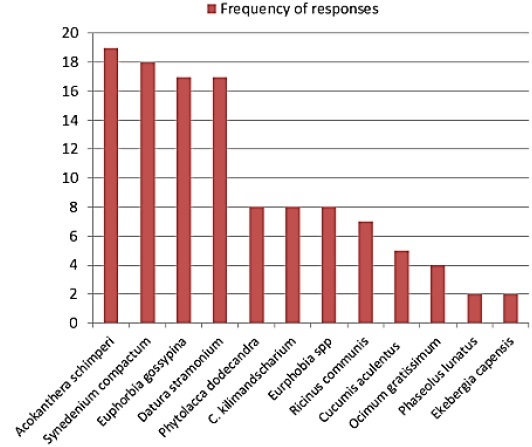
[Table 1.] Plants traditionally used in the management of human diseases in Kenya
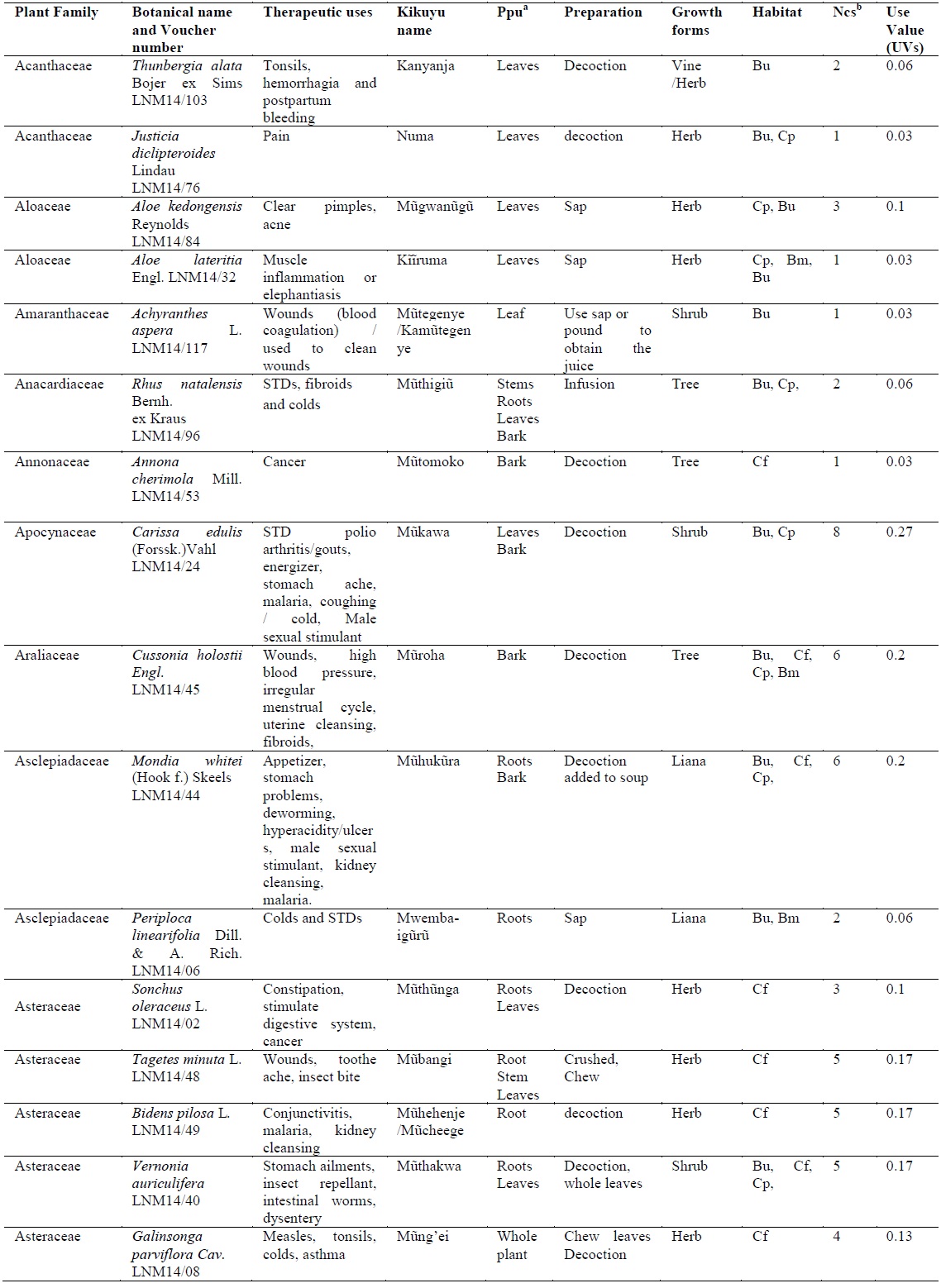
Plants traditionally used in the management of human diseases in Kenya
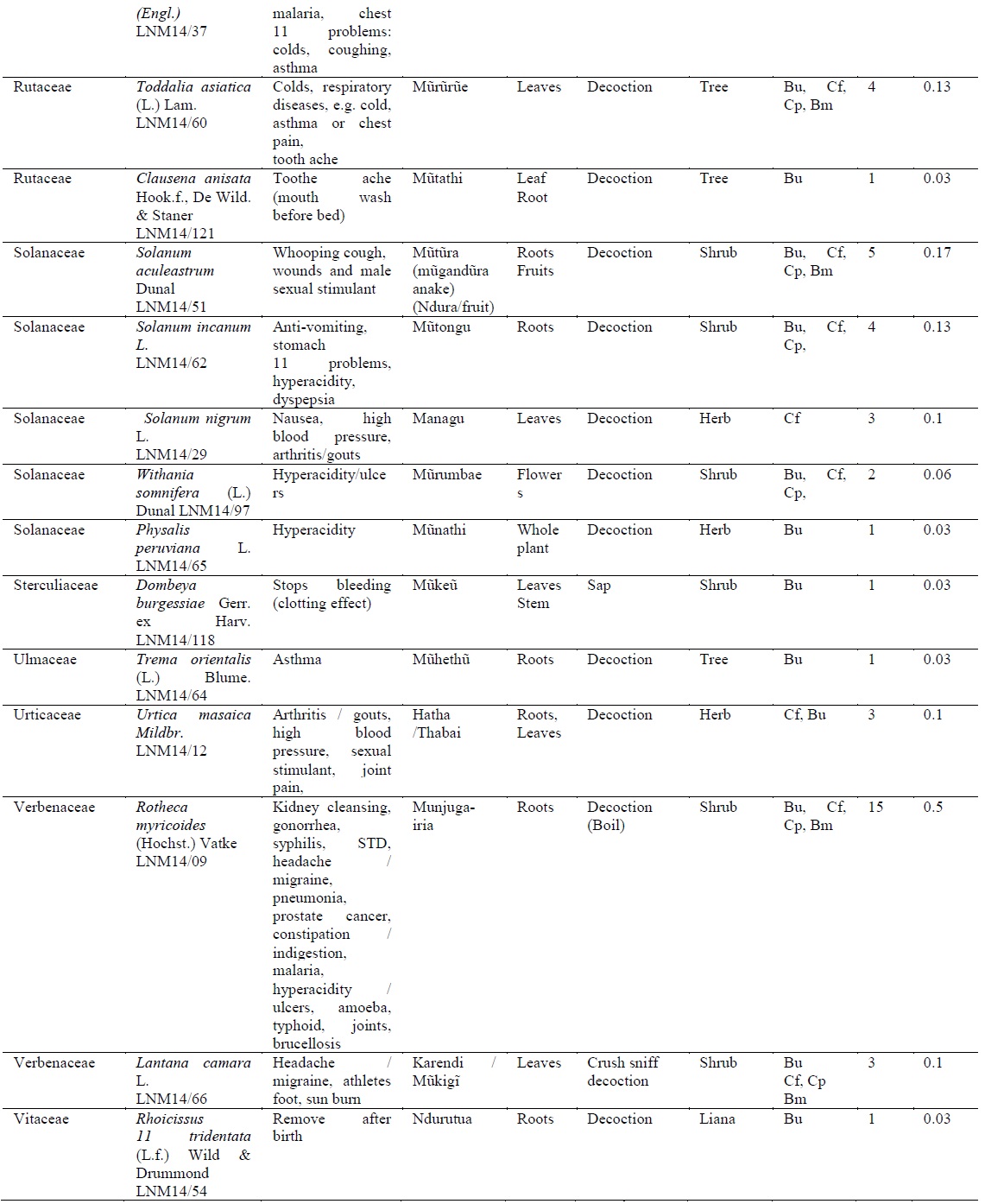
The plants occurred in diverse habitats, 23.8% of the herbs were harvested either from the; bush, crop farms, compound or boundary. The highest proportion of species growth form was trees (36%) followed by shrubs (32%), herbs (24%), liana (7%) and fungi (1%). Regularly harvested plant parts were the roots (34.1%), leaves (25%), bark (20%) and whole plant (9%) (Fig. 2). In order to conserve medicinal plants, the TMPs obtained the bark by cutting longitudinal strips or a third of the roots per plant; others had developed botanical gardens in their farms where they grew trees like
Plant materials were washed and dried before grinding and stored in water proof containers. Plant medicine was prepared by boiling (80%), as an infusion (15%), inhalant or through dermal or nasal application (5%). Frequently used measurement unit was a glass/cup (equivalent to 250 ml) of herbal decoction or infusion taken twice or thrice daily, children took half the adult dose. Preparation was done by the TMP and therefore cases of over dosage were rarely reported, but when they did, the effects included; constipation/indigestion and vomiting which were treated by administering a laxative and anti-vomiting herb respectively. Notably, TMPs did not treat infants, pregnant women, very old people and emergency cases but referred them to hospital for specialized treatment.
Plant toxicity was reportedly rare, however, 11% of TMPs acknowledged that, some herbs like;
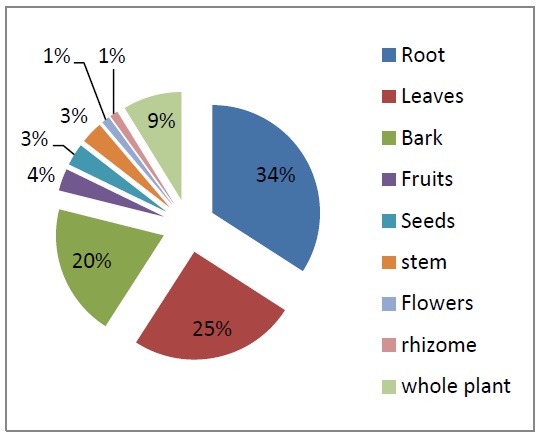
Notably, high level of knowledge in plants that are toxic to both man and animals was observed among the TMPs. Plant(s) that were not eaten by goats or those that produced a milky sap were considered to be poisonous to humans or animals. At least each TMP mentioned 3-5 toxic plants, this finding explained why plant toxicity due to adulteration was reportedly rare; a total of 12 plants were identified and documented (Fig. 3).
The TMPs displayed an in-depth knowledge on herbal medicine used to manage diseases in the Kikuyu community; majority (67%) mentioned over 20 medicinal plants without reference to their records. However, there was no significant relationship between level of education (
Despite their deep knowledge in traditional medicine, the practice faced several challenges, 70% of the TMPs acknowledged that, there was a general belief among members of the community that taking herbal medicine causes resistance to modern drugs. Failure to complete prescribed dose was also reported, especially when a large quantity of herb decoction was administered mainly because the patient presumed that it was an overdose. Other challenges included poor payment for services rendered by the TMPs and very high expectation from the patients for immediate healing.
Majority of the herbalist were old, an indication that the practice was not being passed on to the young generation. This is similar to what was reported in other studies in Kenya (Muthee et al., 2011; Wambugu et al., 2011). Most herbalists were of Christian faith; similar observation was made by Muthee et al. (2011) in Loitoktok District. High level of education among the TMPs was attributed to early introduction of education and Christianity by the missionaries (Sindiga et al., 1995). Lack of laid down structures to pass down knowledge contradicted Kamenju (2013), report which showed that, Kikuyu traditional herbalists undertook the practice as a profession and a means of livelihood and, they routinely passed the knowledge to the young generation. Besides uplifting their confidence and self-esteem in the profession, information acquired from organized seminar had driven out fear among those that had it instilled in them during the colonial period (Sindiga et al., 1995). Additionally, high rate of registration with herbalists’ association was observed in other parts of Kenya, as reported by Muthee et al. (2011) among the Maasai herbalists which were practicing in Loitoktok District.
As observed in the present study, respiratory infections and arthritis have been cited in Tana River County (Kaluwa et al., 2014). Similarly, a study carried out by Bussman et al. (2006) cited a high prevalence of sexually transmitted diseases, malaria, gastro-intestinal disorders, parasitic ailments and wounds among the Maasai of Sekenani. Use of polyherbals in the treatment of diseases is in agreement with Kamenju (2013) view that, Kikuyu traditional herbalists’ treatment approach aims at addressing the root cause of the disease. High usage of shrub and herbs as reported in this study was in agreement with
The present study revealed increased use of roots, similarly, a high prevalence in harvesting of roots and bark was reported among the Ilkisonko Maasai community (Kimondo et al., 2015). But in a study carried out in India by Kumar and Bharati (2014), it was observed that, leaves (33 instances) were the most frequently used plant part. Although root harvesting threatens plants species, conservation measures undertaken by the TMP in the present study area were significant towards protection of the ecosystem. Measurement of the plant medicine using a cup /glass was also observed by Muthee et al. (2011). TMPs in the present study did not treat some groups of patients, the findings contradicted the perception and attitude by pregnant women in Nigeria who believed that, herbal medicine was safe (Fakeye et al. (2009) however, it was in agreement with the report by Muthee et al. (2011).
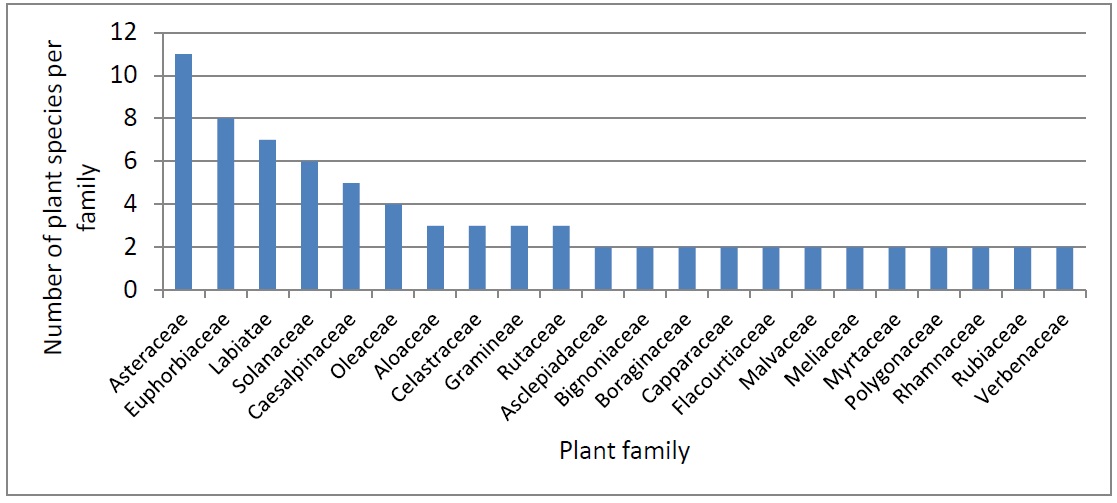
The present study revealed that, the TMPs possessed in-depth knowledge on herbal medicine; similar findings were reported from Samburu County and Sekenani valley in Maasai Mara (Bussman, et al., 2006; Nanyingi et al., 2008). In the present study, family Asteraceae had the highest citations of medicinal plants, this finding concurred with that of Malik et al. (2015) in a study carried out in Northern Punjab. As indicated in the present study, Njoroge (2012) had reported Prunus africana and Strychnos henningsii as frequently used herbs in Central Kenya. TMPs from drier parts of Nyeri County demonstrated deeper knowledge in medicinal plants and reported increased use of herbal medicine by the TMPs. Over reliance on medicinal plants was reported in other drier regions like Samburu and Tana River Counties which had fewer medical facilities (Nanyingi et al., 2008, Kaluwa et al., 2014). The most cited medicinal plants demonstrated various pharmacological activities as well as phytochemicals (Table 2).
[Table 2.] Cross-reference of most cited medicinal plants using existing literature
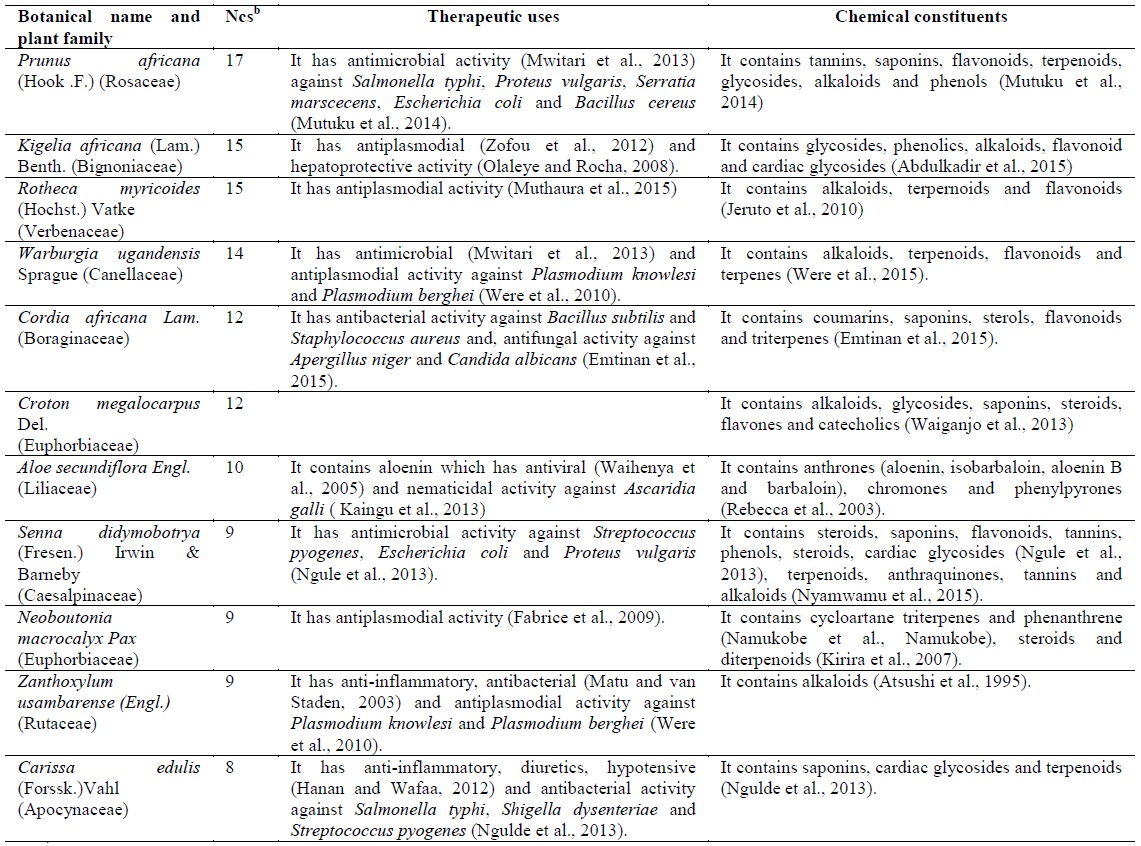
Cross-reference of most cited medicinal plants using existing literature
Major challenges facing demand for the services from TMPs in Nyeri County was attributed to poor perception towards herbal medicine. A study carried out in Thika and Nairobi by Njoroge (2012), showed that, “part of the local populations still holds TMPs with suspicion, erroneously perceiving them as “witchdoctors”. In a study carried out in Murang’a, 20 % of patients didn’t believe that herbal medicine work while 16% said they didn’t like it (Mwangi and Gitonga, 2014). This was in contradiction with the upward trend in the use of traditional herbal medicines observed in other parts of Kenya (Mboya, 2003).
The study concluded that; the current cohort of traditional medicine practitioners from Nyeri County possess vast information about treatment various ailments affecting its community; despite lack of clientele. The documented plants had medicinal potential; the most cited herbal medicines contained common phytochemical compounds such as; terpenoids, flavonoids and saponins and demonstrated pharmacological activities such as antimalarial, antibacterial and antifungal activities. Therefore the study recommended massive campaign about the benefits of herbal medicine in order to promote their use. Further research on efficacy and safety of the documented herbs was encouraged with the aim of developing drugs that can be used to treat and manage various diseases.
The authors declares that there is no conflict of interest