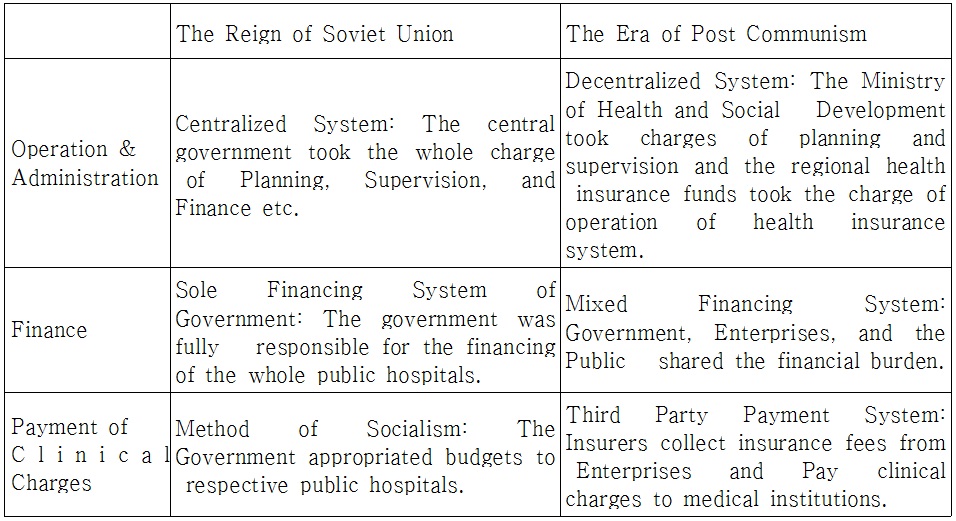
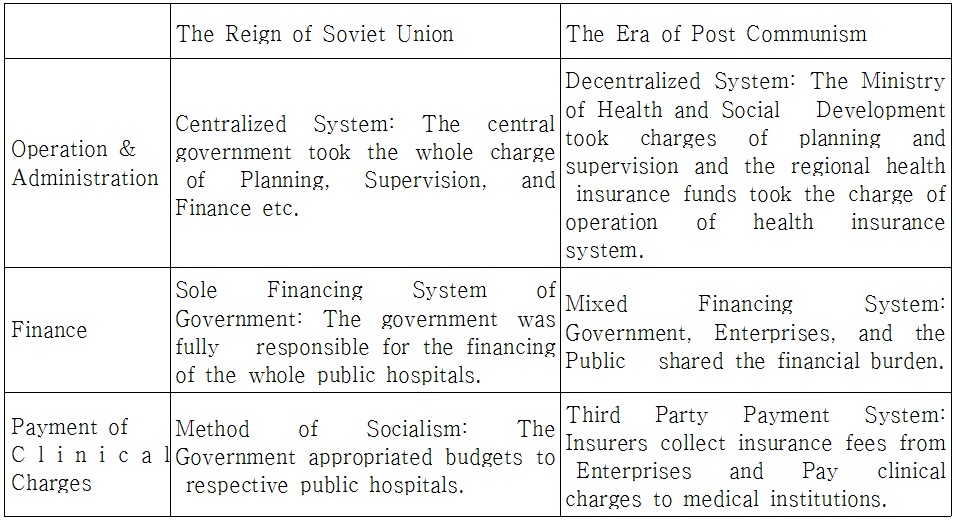
After the collapse of communism, Russia has reformed health care, pensions and social assistance systems. While the reforms of pensions and social assistance systems were stagnated by the Soviet privileges’ resistance, the health care reforms were well proceeded without troubles. The health care reforms focused on the administration systems. The main changes are as follows; First is administrative decentralization. It was changed from the centralization system which central government controlled all aspects of health care system to the decentralization system that central government plans and guides health care system and the local health insurance funds manage the health insurances. Second is the mixed system of financing. The governmental financing system was substituted by the mixed financing system which governments (budgets), enterprises(pay-roll taxes) and citizens(cost sharing) contribute together. Third is the third-party payment system. The socialist system which government directly gave budgets to the public hospitals was transformed to the insurance system which the third-party insurer gathers the contributions of governments and enterprises, and pays medical treatment fees to hospitals. These changes mean the rigid state monopoly system was changed to the mixed system which government and civilians co-share the responsibility of health care system. Under liberal society, it was a inevitable transformation.
Since the dissolution of Soviet Union in 1991, the Russia carried out the welfare reform together with the economic reform shifted from the state-planned economy to market economy. The privatization which was the core idea led the economic reform also applied to the welfare reform. In this welfare reform, the reforms in healthcare, social assistance, and pension were the representative three reforms.1 Compared to the reforms in pension (2003) and social assistance (2004) led by Putin’s Government (the representative welfare reforms in 2000s), the reform of healthcare (1993) was led by Yeltsin’s Government (the representative welfare reform in 1990s).
Contrary to reforms in pension and social assistance proceeded slowly, the healthcare reform promoted in rather early times without disturbances. Reforms in pension and social assistance encountered with strong resistance of vested interests of pension recipients and old Soviet privileged class had been delayed for quite a long period of time however, the healthcare reform proceeded well because it introduced the health insurance by sustaining the existed national medical institutions and officials (=medical service providers) and the fees for medical cares were ascribed to enterprises that evaded the discontent of public.
The healthcare reform changed the existed healthcare administrative system completely. The biggest change was the replacement of conventional free healthcare system with health insurance system. The guaranteed free medical care system through national medical institutions was changed into the third party payment system of health insurance through health insurance fund and private health insurance companies. It was an unavoidable choice to reduce the healthcare budget of government (Manning and Tikhonova eds. 2009).
Transition of state monopolistic healthcare system into the cooperative system of public institutions and private sectors would be a major change in the administrative system. Entry of foreign hospitals and foundation of private hospitals were allowed in the monopolistic system of healthcare provided by national public hospitals that eventually led the previous system into ‘public-private cooperation system’. This was a way intended the successful introduction of health insurance system and to improve the quality of healthcare service.
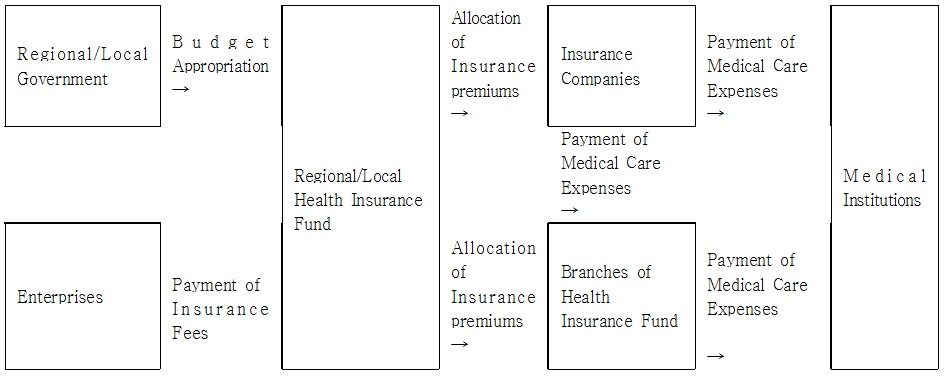
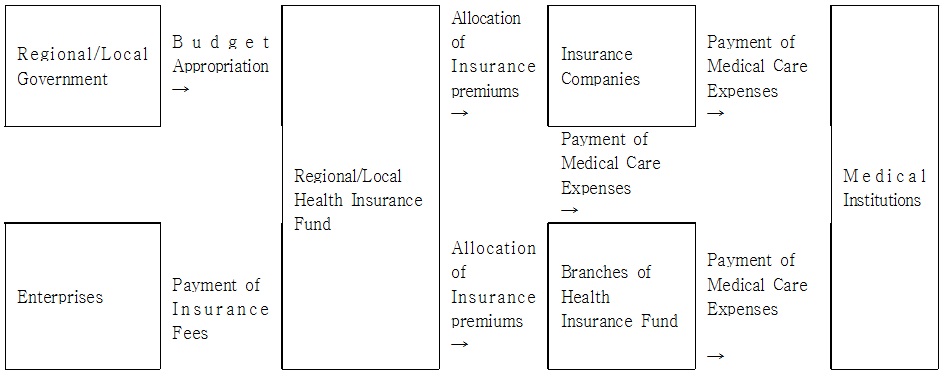
The most obvious feature of healthcare reform in Russia would be the build-up of public-private mixed system. Private insurance companies were supposed to participate in health insurance funds to collect insurance expense and to pay charges of medical care together as an insurer (the 3rd party); and the private hospitals were allowed to provide the public with shared health care services of national and private hospitals.
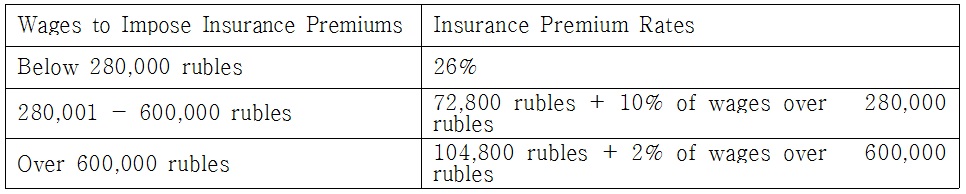
The ‘public-private mixed system’ implies the reduction of government’s role to provide healthcare services (national hospitals in the Soviet Union solely provided healthcare services with dedicated finances). The share of finances for health insurance (insurance expenses of employees and non-employees were supposed to be paid by private enterprises and government), the permission of foundation of private hospitals, and the participation of private insurance companies as an insurer in health insurance funds were all measures to reduce government’s role and to expand the role of private sectors instead (Chubarova, 2003: 3).
In this paper, it was intended to examine the changes in administrative system along with the healthcare reform in Russia situated in the era of post communism. The consecutive changes from previous healthcare system of Soviet Union to the reform of healthcare system after the dissolution of Soviet Union will be described along with examinations on the background of introduction of health insurance system and related issues; and based on this further issues and corresponding alternatives will be presented.
Ⅱ. Healthcare System in Russia
1. Healthcare System in Soviet Union
Public medical institutions were introduced as one alternative of the reform of liberalism under the reign of the Alexander II of Russia in 1864. Initially, it aimed the cure of diseases of the poor in country sides. Accordingly, clinics and hospitals employed medical doctors were founded. And local governments took corresponding financial burden to provide free healthcare services. In 1890, 16% of medical doctors in Russia worked in the local medical institutions. Along with the increase of the number of urban laborers on the track of industrialization, the health insurance similar to social insurance system introduced by Bismarck (1815~1898) was also introduced for the first time, and it covered about 20% of industrial laborers.
The Soviet Government entered after the Russian Revolution in 1917 established the free national healthcare system to cure and to prevent diseases. The free healthcare system was one of major national functions in the Soviet country. The national responsibility, free healthcare service, importance of prevention of diseases, intensification of the specialty of medical care, scientific medical examinations and treatment, health promotion, and the continuation of treatment and rehabilitation were the principles of the single Soviet health care system wholly controlled and run by the government.
In 1927, the social insurance fund was dismissed and the finances were absorbed into government budget. And all hospitals, pharmacies, and other medical institutions were nationalized. Then the nationalized medical institutions were situated under the direct administration of local healthcare bureaus. Required finances were appropriated from the central government budget and all healthcare human resources became public officials. Thus the complete national control system over public healthcare was established (Chubarova, 2003: 3). And in 1936, the People’s Commissariat of Health was founded to administrate overall issues on public healthcare.3 Special hospitals under direct management for certain occupations such as leading group of Communist Party, high class officials such as in Defense Department or Public Security Department, mine workers, workers in heavy industry, and laborers in railroads were also introduced (Grigorieva, 2012:3).
In the meantime, doctors in the Soviet country were regarded as national workers. Governments of each republic composed the Soviet Union hired medical doctors and paid respective wages. Contrary to doctors in Western countries, they treated patients as members of respective community according to ‘Red Medicine’, and were obliged to maximize the labor efficiency of patients by promoting patients’ health. They thought that healthy people would make health nation as the invalid would make respective country invalid. Medical doctors placed in urban area prioritized the cares for factory workers constituted the backbone of Socialism compared to other patients in families, hospitals, or clinics. Level of compensation for medical doctors in Soviet countries were low. The level was equivalent to the level of teachers in elementary schools which was a little bit more than those of nurses. Compensations for medical doctors working in the primary, secondary and tertiary medical institutions were equivalent (Tragakes and Leggof, 2003: 167).
2. Healthcare System in the Era of Post Communism
Since the dissolution of Soviet Union in 1991, no significant changes have been made in quantitative and qualitative aspects of medical institutions. Above all, the extensive privatization in socio-economic fields have been accomplished since then except the medical institutions remained as public properties. The quantitative scale of Russian medical institutions and medical service providers is still quite significant. In 2010, there were 5,993 hospitals, 7,951 public health clinics, 2,330 ambulatory clinics, and 827 dental clinics from which numbers of sickbeds were relatively plentiful compared to current population. In 2008, number of medical doctors and nurses in Russia were 621,000 and about 1.3 million respectively. Average number of medical doctors was 42.8 per population of 10,000 people while it was 12.1 for the case of country sides.4 In spite of the significant gap of numbers of medical doctors between urban and rural area the average numbers of medical doctors, medical specialists, interns, dentists, nurses, and pharmacists per one people exceed those of EU. Levels of current medical services have been remaining almost the same since those realized in the era of Soviet Union. And the level of quality of medical service and compensation for doctors are still low. There are no established patients transfer system between local governments and no competition between each hospital. Payments for medical charges of patients resided outside of current region would be refused by local health insurance funds. And funds for the research in respective hospitals are rare (Davydov and Shepin, 2010:74-76).
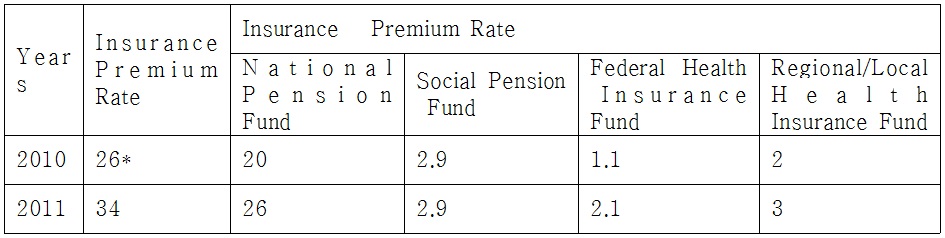
However, big changes have been made in the fields of financing and transfer of finances in healthcare system. In 1993, the mandatory health insurance was implemented, and in 1998, the free healthcare services to all the people was initiated (by government budget) and around 2005, the independent health insurance funds were established. With the introduction of health insurance system, the major source of finances for hospitals were moved from government budget to health insurance funds. Financial resources for hospitals consists of ① compensations for medical service providers, expenses for medicines, clothing and meals for patients paid by local health insurance funds and insurance companies ② investment expenses for hi-tech services (medical equipment etc.) and expenses for facilities maintenance and operation paid by local government, ③ fees for medical care paid by insurance companies, and ④ self-charged amount paid by each patient (World Bank, 2011: 20).
Together with such changes, the entry of private hospitals would be one of significant changes. With the coming of 1990s, the foundation of private hospitals was allowed along with the private insurance companies. From the one dental clinic opened in Moscow for the first time, there are currently about 2,000~3,000 dental clinics in Moscow. Annual number of clients visited to private hospitals reached up to about 4 million. Besides dental clinics there are many ophthalmic and health examination clinics among private institutions. Private pharmaceutical companies have also appeared. Expenses for medicines have been excluded from insurance benefit thus the privatization of pharmaceutical companies have been advanced (Tragakes and Leggof, 2003: 41).
In 1999, chain of foreign hospitals opened one hospital in Moscow. Rich people typically visit private hospitals charging expensive fees for medical cares. Costs for medical cares are normally calculated by ‘fee for service’ basis and paid directly by patients. In 2008, there were about 30,000 private hospitals but few of them participated in the mandatory health insurance. About half of the services of medical care provided by private hospitals would be covered by health insurance benefit. For the case of dental care, only the basic medical cares were supposed to be covered by health insurance benefit and elsewhere it would be the self-charged amount of patients. Due to this self-charged amount the profit-making hospital can secure the ground for its foundation (World Bank, 2011: 27).
On the other hand, large-scaled enterprises or medium sized corporations make contracts with hospitals for respective employees or operate hospitals of their own under direct administration. The quality of free medical services from such hospitals are typically higher than those from national hospitals. About 30% of the whole population take medical services from such hospitals. Police officers, staffs of railroad administration or universities, and high class officials use dedicated hospitals free of charge. Doctors in Russia have been kept the status of public official since the dissolution of Soviet Union and most of them are working in the national/public (local) medical institutions (hospitals) (Teplova, 2007: 315).
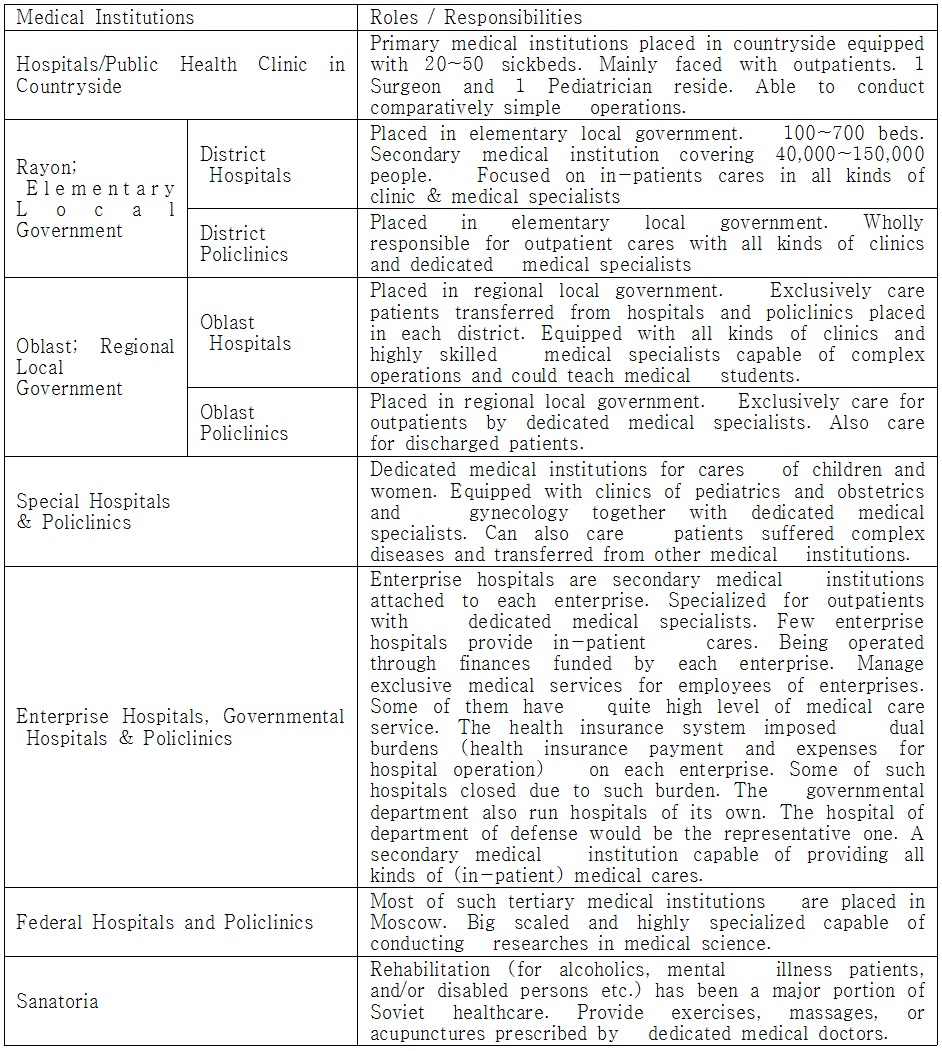
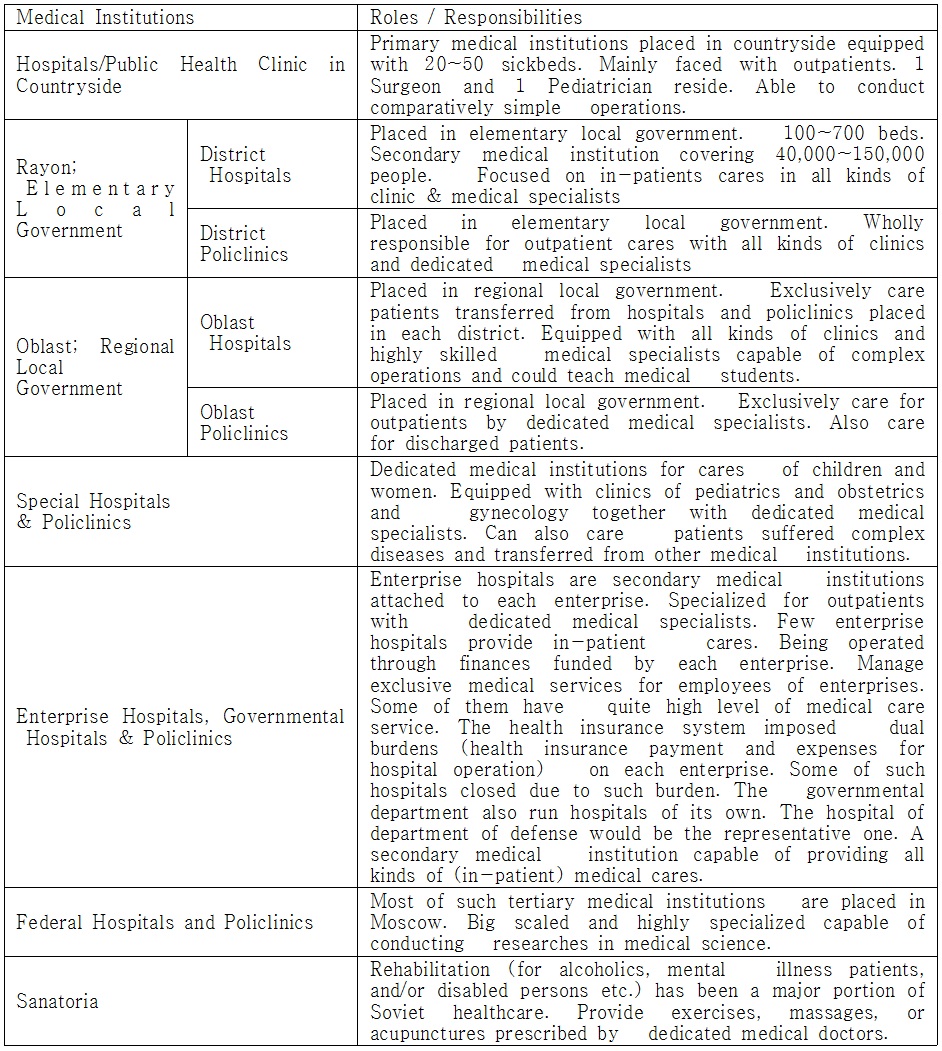
Types of the roles of medical institutions which have been maintained its basic framework since the dissolution of Soviet Union can be classified into following. The ‘hospital/public health clinic’ placed in countryside typically consists of 20~50 beds as a primary medical institution. Each one of pediatrician and surgeon in such institution would be mainly faced with outpatients. They can conduct comparatively simple surgical operations. The ‘district hospitals’ placed in each rayon of Russia would be secondary medical institutions typically consisted of 200~500 beds. One such hospital would usually cover the population of 40,000 ~ 150,000. It typically provides inpatients with medical cares and equipped with almost all kinds of clinics with corresponding specialists.
The policlinics in each district5 would be placed in elementary local government and has all clinics and specialists dedicated for outpatients. The oblast hospitals are placed in each oblast (=the regional government). The hospitals typically cares patients transferred from hospitals or policlinics of each district. Such hospitals typically equipped with all kinds of clinics with high level specialists. They can conduct complex operations and teach medical students. Policlinics in oblast is a medical institution specialized for outpatients typically care for patients discharged from hospitals. Special hospitals or policlinics may be the medical institutions specialized for children or women equipped with groups of specialists in pediatrics and obstetrics and gynecology. They can also care patients suffered complex diseases and transferred from other medical institutions.
Enterprise hospitals, governmental hospitals, and policlinics are secondary medical institutions attached to each enterprise or government ministry and/or offices. They are also specialized for outpatients with dedicated medical specialists. Few enterprise hospitals provide in-patient cares. They manage exclusive medical services for employees of enterprises or workers in government ministry and offices through finances funded by each enterprise. Some of them have quite high level of medical care service. With the implementation of health insurance system enterprises have to bear the dual burdens of health insurance payment and expenses for operations of hospitals under direct management. Some of them gave up the operation of hospital due to financial difficulties. The hospital directly managed by department of defense would the representative governmental hospital. The hospital is a secondary medical institution that provides all kinds of medical care services.
The Federal Hospital and Federal Policlinic are tertiary medical institutions and most of them are placed in Moscow. They are big scaled and highly specialized. They can also conduct researches in medical sciences. The sanatoria wholly responsible for treatments and rehabilitation mainly cares for alcoholics, mental illness patients, and disabled persons. Proper exercises, massages, or acupunctures prescribed by dedicated medical doctors are provided.
In the meantime, the remuneration reform in public sector of Russia was carried out in 2008.6
It was an introduction of the elastic new remuneration system (NRS) emphasized the relationship between performance and compensation which had been employed in the business sector, and thereby extended to hospitals. By this reform, the principal medical doctor was endowed with the right to raise or lower the level of compensation of individual doctors in the extent of the whole amount of remuneration. Thus doctors and nurses manifested high performance or productivity can get more rewards (performance fee). However, effects of such incentive reinforcement in healthcare sector revealed by performances before and after the reform are still uncertain, and it has been estimated that it could be attributable to the resistance against the reform (Kolosnitsyna, 2012: 118).
Yeltsin’s Government well recognized that the running of Soviet National Healthcare System in the society of post Communism would be impossible due to financial limit. Accordingly, issues of the reform of healthcare system was put on tables except the model of laissez-faire supposed the individual payment of medical care expenses.