Adolescent menorrhagia is defined as excessive menstrual bleeding from menarche to adolescents. It is a distressing condition both for the patient as well as for her parents. If it is not managed in time itmay pose significant health problems that may leads to blood transfusion. We determined the efficacy of Geru (Red ochre) in controlling the amount and duration of blood flow in patients of Adolescent menorrhagia. This study included 40 teenage girls, who presented with heavy bleeding during menstruation to Outpatient Department, Sameena Maternity Nursing Home, Hyderabad during the year of 2013. Assessment of each case was done by history and Pictorial Blood loss Assessment Chart (PBAC) score. Geru powder was given for 2 cycles and results were assessed. The data was analyzed statistically. The mean PBAC score before treatment was 497.04 ± 389.92and after trial in 1stand 2ndit was found to be 471.13 ± 162.18 and 310.13 ± 142.15 respectively. On basis of results it was concluded that single unani drug Geru is enough in controlling bleeding and was found effective by its astringent and styptic properties.
Gynecological problems of adolescents occupy a special place in the spectrum of gynecological disorder of all age groups especially puberty menorrhagia. Adolescent or Puberty menorrhagia is defined as excessive bleeding in amount more than 80ml or in duration more than 7days between menarche and 19 years of age (Caufriez A, 1991; Hallberg et al., 1966). The prevalence of Adolescent menorrhagia is estimated about 75% of all adolescent problems. Almost a quarter of population in developing countries comprises girls below 20 years of age. In India; children less than 15 years of age constitute about 40% of population (Park, 2022). Menstrual disorders affect 75% of adolescent females and are a leading reason for visit to physicians (Gail, 2003). During this period, it is common for adolescents to present with complaints of menstrual irregularities. The onset of menstruation is influenced by a number of factors like genetics, nutrition, body weight and maturation of the hypothalamic pituitary ovarian axis. The onset of menstruation does not mean that ovulation is occurring. In the majority, early menstrual cycles are anovulatory (Lemarchand-Béraud et al., 1982). The cycle length varies for some considerable years after menarche. It may take some 5-8 years to establish regular menstrual cycle. During this time it is common for adolescents to present with menstrual irregularities (Hallberg et al.1966; Lemarchand-Béraud et al., 1982).The most common cause of Adolescent menorrhagia is anovulatory cycles, which are related to immaturity of the hypothalamic-pituitary-ovarian axis (Claessens and Cowell, 1981; Falcone et al., 1994).
There is an immaturity of the hypothalamus and negative feedback results in sustained high levels of oestrogen. An organic disease or malignancy in particular, is very rare. Heavy, irregular menstrual bleeding is a frequent complaint in adolescent girls. The prevalence of menorrhagia in adolescent populations with bleeding disorders varies between 14 to 48%. It is likely to be caused by mechanisms which are different from those which occur in women in the fourth or fifth decades of their life, where anatomic causes of bleeding are common (Bevan et al., 2001; Brenner, 1996; Hickey and Balen, 2003; Rao et al., 2004; Roychowdhury et al., 2008).
Anemia is a potential squeal of Adolescent menorrhagia (Revel-Vilk et al., 2012). This squeal may be prevented with appropriate management of the underlying problem. Therefore, it is important to establish the correct diagnosis before any therapy is administered. In conventional medicine the interventions used to reduce menstrual blood flow are by using hormones like combined oral Contraceptive (COC) pills, Gonadotrophin-Releasing Hormone (GnRH) analogues and oral progesterone.
In unani system of medicine in almost all classical text causes, clinical features, complications and treatment of menorrhagia are mentioned, but particular mention about puberty menorrhagia is not made. According to unani physicians the causes of menorrhagia are
Menorrhagia may be due to
There is poor correlation between a woman’s perception of heavy menstrual bleeding and menstrual blood loss of more than or equal to 80 ml and between the number of sanitary pads used and the complaint of heavy bleeding (Janssen et al., 1995). Hence Pictorial Blood Loss Assessment Chart (PBAC) was used for the assessment of the results. The objective of the study was to evaluate the effect of
The present clinical study was carried out in Outpatient Department, Sameena Maternity Nursing Home, Hyderabad during the year of 2013. The study population comprised of 40teenage girls from 13 to 19 years of age with historyof prolonged/heavy bleeding during menstruation.The detailed history regarding the age, age at menarche, duration of cycle, duration of flow, amount of flow, passing clots, number of pads required dailyand pain abdomen were recorded.Assessment of blood loss during menstruation was estimated by taking detailed history of using sanitary pads per day.
Regarding the assessment of blood flow patients were given a pictorial blood loss assessment chart (PBAC) along with verbal instructions onhow to fill the chart. PBAC is a simple scoring system. It takes into account the number ofsanitary pads used per day and the degree of their soiling.The pictorial assessment chartwas scored before and after trial as described by Higham et al (1990). The cutoffpoint 180 was most appropriate for diagnosing the menorrhagia, in this study cases with PBAC score of more than 400 were included and treated.Results were analyzedstatistically.
Design: Before and after treatment
Sample size: 40 unmarried girls
Inclusion criteria: 13 - 19 years with prolong orheavy blood flow
Test drug:
Duration of treatment: For 3 days starting from1stday of cycle, 3 gm of powder for oral use with water twice a day for 2consecutive cycles
Assessment of results: By relief of symptoms andPBAC Score
The drug
Studies have been carried out on different astringent and styptic drugs like
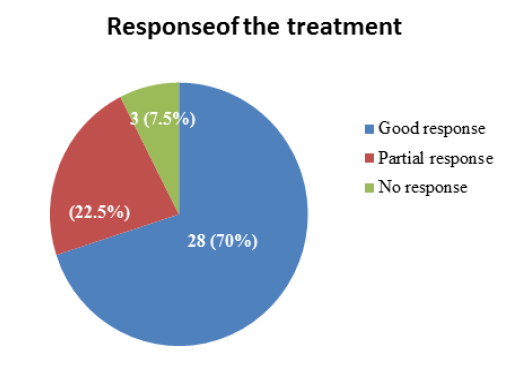
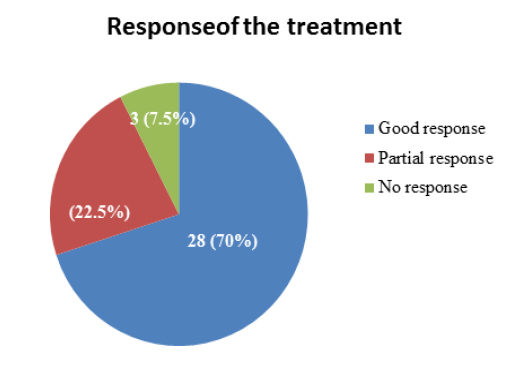
In this study total 40 adolescent girls were treated with single drug
It was concluded that Adolescent menorrhagia is a common disorders among teenage girls. It is a major problem that poses severe heath consequences requiring blood transfusion. Medical management is effective in most of the cases. Unani drug