Yoga is an ancient Indian system of life, encompassing various practices including practices for self-discipline and also for regulating the health states of the individual, being practiced for thousands of years. The present study aims at understanding the effect of two high frequency breathing practices over autonomic nervous system. Forty healthy male volunteers of age 21 ± 2 years with 9 ± 3 months of Yoga practice experience were recruited. The two high frequency Yoga breathing practices, kapalabhati (KB) and bhastrika (BH) were given as interventions randomly on either of the two days to minimise laboratory bias. They were assessed before and immediately after the interventions for heart rate, respiratory rate, heart rate variability (HRV), blood pressure and peripheral oxygen saturation. There was a significant increase in heart rate (p < 0.01; p < 0.001), systolic blood pressure (p < 0.01; p < 0.001), NN50 (p < 0.01; p < 0.001) component of HRV for both KB and BH groups respectively. There was a significant reduction in respiratory rate in both the groups (p < 0.001, and p < 0.05, BH and KB respectively) immediately following intervention. A significant increase in LF component of HRV and reduction in Diastolic blood pressure and high frequency (HF) component following KB was also observed (p < 0.05, for all comparisons). The Mean peripheral oxygen saturation remained unaltered in both the groups (p > 0.05). The results suggest that high frequency yoga breathing practices induce physiological arousal immediately as evidenced by increased blood pressure and heart rate. The sympathetic arousal was more following KB session as evidenced by an increased diastolic blood pressure, LF power and a decrease in HF power of HRV as compared to the BH session.
Present day science has started recognizing the relationship between the emotional regulation, breathing and metabolism (Porges, 2001), which has been described in the
However, there being very subtle difference in the actual procedure of the practice, these practices have been described as voluntary breath regulation practices and cleansing procedures thereby demanding closer observation into the traditional literatures to unearth their significance and understand their possible applications.
Experimental data shows that KB and BH practices have a direct influence on physiological processes such as respiratory and cardiovascular system, biochemical parameters (Desai and Gharote, 1990) and central nervous activity (Stancák et al., 1991). An increase in the performance in a letter cancellation task was observed immediately after practice of KB at a rate of 60 strokes (breaths) per minute (Telles et al., 2008). Whereas the cognitive evoked potentials showed a reduction in latency and increase in amplitude following practice of KB when administered at the rate of 120 strokes (breaths) per minute (Joshi and Telles, 2009). Earlier studies have reported that slower breathing practices, alternate nostril breathing (
Heart Rate Variability (HRV) is an indicator of the autonomic nervous system activity of an individual. Previous studies conducted on the influence of
Subjects
An advertisement mentioning ‘volunteers shall register for a study to understand the autonomic regulations of two breathing practices’ was made in a residential
Subjects were assessed five minutes before and immediately after KB on one day and BH on another day, but at the same time of the day with similar physical mental load before coming to the laboratory. Alternate allocation of KB and BH on day one of their visit to the lab was done to ensure 50% of the subjects performing KB on Day one while the remaining 50% performed BH.
Immediately after reaching the laboratory, subjects were made to sit in a sound attenuated, dim light room, allowing them to relax for five minutes, following which baseline recordings of blood pressure, heart rate, ECG, oxygen saturation, and respiration were recorded. The intervention KB and BH were randomly administered for duration of 1 min.
Heart Rate Variability
The ECG was recorded using a polygraph (BIOPAC MP100, USA) at a sampling rate 1024 Hz and was analyzed offline. The data were acquired using the standard limb lead II configuration in five minutes epochs before and immediately after the intervention. The data was visually inspected offline and noise free data were included for analysis. The R data waves were detected to obtain a point event series of successive RR intervals, from which the beat to beat heart series were computed. The data were analysed with an HRV analysis program, ‘Kubios’, developed by the biomedical signal analysis group (Finland).
Respiration (R)
Respiration was as recorded using a stetho-graph fastened approximately 1 cm below the margin of the rib cage while subject was made to sit erect. Respiration was constantly monitored before and immediately following the intervention for 5 mins.
Blood pressure (BP)
A digital sphygmomanometer device (Mindray, Hong Kong) was used to monitor the blood pressure. The digital manometer was tied in the left arm over the brachial artery and was inflated to record the blood pressure immediately before the start and after the completion of the intervention.
Oxygen Saturation
Oxygen saturation was measured using Pulse oxymeter (Mindray, Hong Kong). A photo plethysmograph comprising of an infra-red diode was connected to the middle finger of the right hand and continuous blood oxygen saturation was recorded before and after the intervention for five minutes.
Intervention
The participants were made to sit in a chair having their spine straight and the hands resting on the knees. With their eyes closed, they were asked to voluntarily relax the entire body. Ag-AgCl electrodes were placed as per limb lead II and respiration belt was applied on the chest 1 cm below the lower margin of the rib cage. Sphygmomanometer cuff was tied to the left arm and the Pulse Oximeter was fixed to the thumb of the right hand to avoid any interference from the sphygmomanometer cuff.
KB and BH was administered as mentioned in Hatha
KB: The participants were asked to sit in a chair having the spine straight and the hands resting on the knees. The subjects were instructed to relax the whole body. Inhaling deeply through both nostrils, expanding the abdomen, the subject has to exhale with a forceful contraction of the abdominal muscles. Following forceful exhalation, voluntary relaxation of the abdominal muscles promotes downward movement of the diaphragm causing a negative pressure in the thoracic cavity, facilitating rapid influx of air. The speed of the practice was guided with the help of an electronic timer device. After completion of 60 rapid breaths in succession, the participants were asked to relax in the same position without voluntarily manipulating their breath. (Muktibodhananda, 2000).
BH: The subjects were instructed to breathe in and out forcefully through the nose without straining any part of the body. Inhaling deeply through both the nostrils forcefully, the subjects were instructed to exhale forcefully for 40 rounds in a rhythmic fashion. The speed of the practice was guided with the help of an electronic timer device. (Muktibodhananda, 2000).
Statistical analysis
Statistical analysis was performed using the SPSS version 19.0. Following the normal distribution of the data as indicated through Shapiro–wilk’s test, within group differences were analyzed using paired ‘
Paired ‘
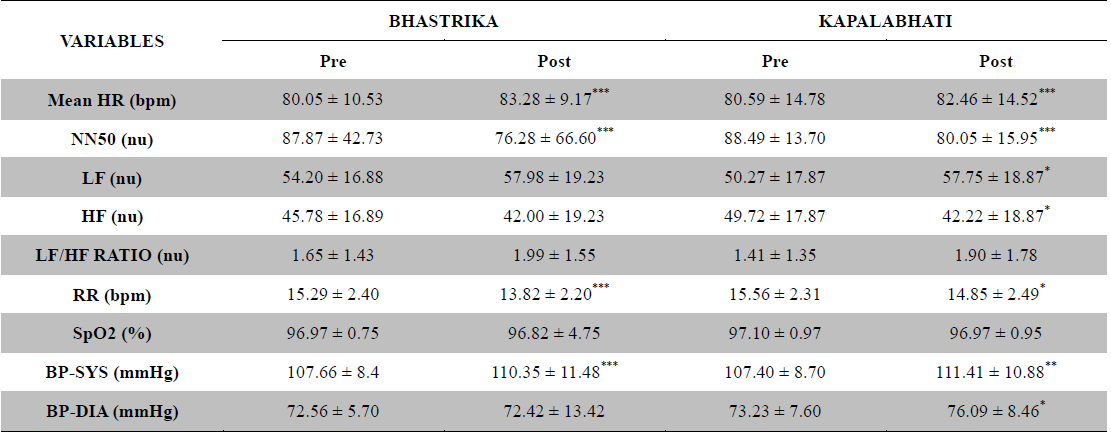
Respiratory rate was significantly reduced immediately following both the practices KB (
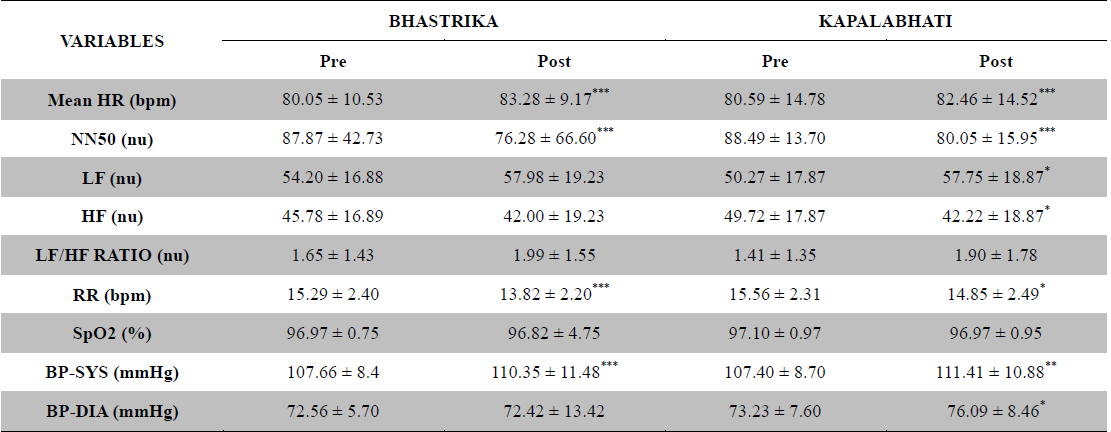
The group mean ± SD of HRV, SpO2, RR and BP recorded before and immediately after the practice of Kapalabhati and Bhastrika Pranayama
The purpose of this study was to understand the influence of two High Frequency
The findings of the present study are in accordance with the earlier findings indicating an increase in Sympathetic Nervous System activity immediately after both the practices. However, the sympathetic arousal was non-significantly more following the practice of BH as compared to KB, which can be attributed to the increased effort required to perform the BH, requiring more Cardiac output to suffice the needs of the exercising respiratory musculature and the diaphragm.
High frequency breathing is known to cause a direct influence on physiological processes through the cardio respiratory system (Stancák et al., 1991).
Though KB was shown to be a stimulating practice, reported to improve attention and concentration (Tells et al., 2008), there was a need to understand simpler breathing based methods to increase sympathetic activity. It is clear from the present study that high frequency breathing has a direct impact on the autonomic nervous system. While BH showed more influence on blood pressure and heart rate, KB had better influence on heart rate variability as expected. BH practice appears to influence the cardio Respiratory system more mechanically than KB.
The thoraco-abdominal manoeuvring involved in BH results in increased breath volume and greater contraction and expansion of the thorax and abdominal wall. In comparison, KB with more of diaphragmatic movement appears to exert less mechanical pressure on the thorax and hence has less influence on the blood pressure. No changes observed in oxygen saturation levels can probably be attributed to the duration of the practice.
The findings of the present study are in accordance with the earlier findings of high frequency breathing practices directly regulating the autonomic nervous system. The results suggest that practice of