This study used semiology based on traditional Chinese medicine (TCM) to investigate vital energy (Qi) behavior in women with abdominal myofascial pain syndrome (AMPS).
Fifty women diagnosed with chronic pelvic pain (CPP) secondary to AMPS were evaluated by using a questionnaire based on the theories of “yin-yang,” “zang-fu”, and “five elements”. We assessed the following aspects of the illness: symptomatology; specific location of myofascial trigger points (MTrPs); onset, cause, duration and frequency of symptoms; and patient and family history. The patients tongues, lips, skin colors, and tones of speech were examined. Patients were questioned on various aspects related to breathing, sweating, sleep quality, emotions, and preferences related to color, food, flavors, and weather or seasons. Thirst, gastrointestinal dysfunction, excreta (feces and urine), menstrual cycle, the five senses, and characteristic pain symptoms related to headache, musculoskeletal pain, abdomen, and chest were also investigated.
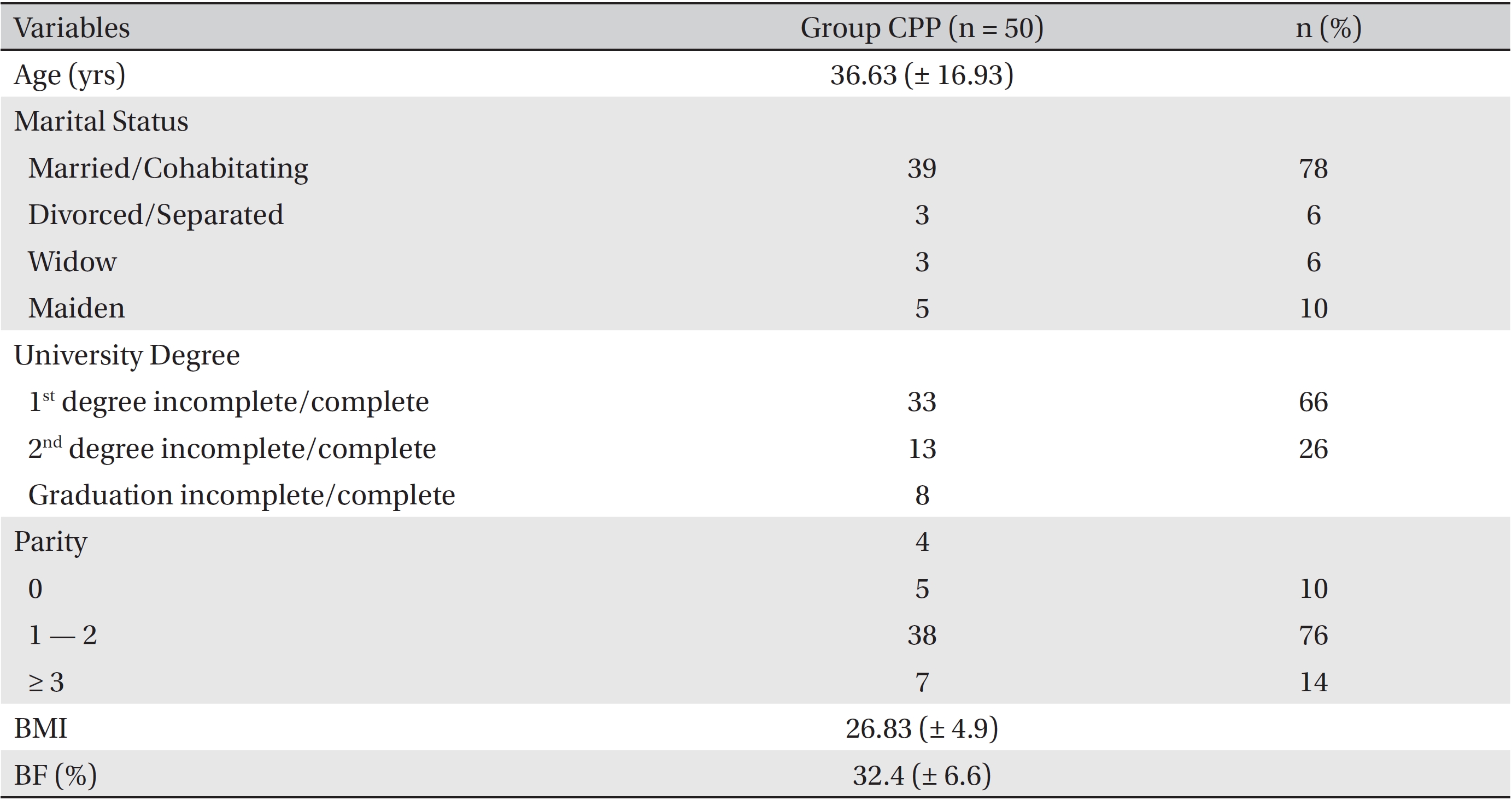
Patients were between 22 and 56 years old, and most were married (78%), possessed a elementary school (66%), and had one or two children (76%). The mean body mass index and body fat were 26.86 kg/ cm2 (range: 17.7 — 39.0) and 32.4% (range: 10.7 — 45.7), respectively. A large majority of women (96%) exhibited alterations in the kidney meridian, and 98% had an altered gallbladder meridian. We observed major changes in the kidney and the gallbladder Qi meridians in 76% and 62% of patients, respectively. Five of the twelve meridians analyzed exhibited Qi patterns similar to pelvic innervation Qi and meridians, indicating that the paths of some of these meridians were directly related to innervation of the pelvic floor and abdominal region.
The women in this study showed changes in the behavior of the energy meridians, and the paths of some of the meridians were directly related to innervation of the pelvic floor and abdominal region.
Chronic pelvic pain (CPP) is defined as non-menstrual or non-cyclic pelvic pain lasting for at least 6 months that interferes with normal activities and requires medical or surgical treatment [1]. According to Gelbaya and El-Halwagy [2], CPP is considered a major health problem for women. In the U.S.A., CPP is responsible for 10% of outpatient visits to a gynecologist, 40% of laparoscopies, and 10% to 15% of hysterectomies [3-5]. Its estimated prevalence is 3.8% in women aged 15 — 73 years [6] and 14% — 24% in women of reproductive age [7, 8], and it has direct effects on civil, social, and professional status. Its etiological model is multifactorial, with several causative factors. Among these etiologies is the complex interaction between the gastrointestinal, genitourinary, musculoskeletal, nervous, and endocrine systems, in addition to sociocultural influences. A growing body of studies has highlighted the importance of the musculoskeletal system in the etiology and persistence of CPP [9]. Strong evidence indicates that up to 85% of patients with CPP have musculoskeletal system dysfunction [10]; myofascial syndrome is one of the anomalies that have been identified.
Abdominal myofascial pain syndrome (AMPS) is characterized as a deep and intense pain in the abdominal region, originating from latent myofascial trigger points (MTrPs) located in the muscles and/or fascia [11]. MTrPs can be classified as either active or latent [12]. Active MTrPs may cause pain at rest and produce referred pain similar to that felt during compression of the point. Latent MTrPs do not cause spontaneous pain, but can restrict movement or cause muscle weakness, and only become sore if they receive direct pressure [13]. In addition to nociceptive phenomena, latent MTrPs may also produce muscle spasm and autonomic phenomena such as piloerection, vasoconstriction, vasodilatation, sweating, temperature changes, and a variety of visceral somatic reflexes [12, 13].
Treatment of AMPS requires a multidisciplinary approach in order to break the cycle of pain, deactivate the MTrPs, and restore muscle flexibility, thereby eliminating predisposing factors and perpetuation of pain [14]. Treatment strategies include behavioral therapy, medications, physical therapy, injections at trigger points, neuromodulation, botulinum toxin injection, and various forms of alternative treatments, such as acupuncture. Traditional Chinese medicine (TCM) techniques manipulate vital energy (Qi) flow through meridians to balance the opposing forces of yin and yang, as well as the five elements [15, 16]. The meridians through which Qi is circulated comprise a succession of points located at anatomically specific sites across different regions of the human body [17], including the lung, heart, liver, spleen, kidneys, and pericardium meridians; the latter is not associated with a specific organ, but involves action on yin Qi and genitourinary function [18]. Other meridians include the large intestine, small intestine, gallbladder, stomach, bladder, and the triple energizer meridians, the latter of which acts on the yang Qi and respiratory, cardiac, and digestive functions. For TCM, and by extension acupuncture, the theories of “yin and yang”, “five elements”, and “zang-fu” are interlinked and advocate an interdependence of humans with nature; these theories are widely observed and applied in clinical practice [18].
In TCM, pain is a result of a blockage or stagnation of the normal movement of Qi in the painful area and is understood to be a consequence of biological-process disruption. Changes in the flow of Qi present symptoms of energy accumulation (yang) or deficiency (yin) in relation to the organs and viscera [19]. If a diagnosis is to be made, the energy imbalance must be recognized by analyzing the individual as a whole based on the categories of the semiological disorder parameters related to pain: sensory, temporal, topographical, factors of aggravation and improvement, and pathophysiological [20]. These can be assessed according to qualitative criteria: surface and depth, that set the standard for pathogenic factors; or quantitative criteria: yin-yang deficiency or yin-yang excess in relation to the internal organs (zang-fu), as well as the musculoskeletal system [21]. Acupuncture is based on a clinical diagnosis that recognizes and groups semiological data on the syndrome to provide clear guidelines for establishing therapeutic measures [22]. The aim of this study was to determine which zang-fu meridians had altered Qi behavior and to determine if yin-yang disharmony existed in the altered meridians in women diagnosed with AMPS through a TCM evaluation.
This study was approved by the ethics committee of the faculty of medicine at the hospital of Ribeirao Preto, university of São Paulo, and patient consent was obtained. This study included women with a clinical diagnosis of CPP, secondary to AMPS, who visited the clinic of gynecological endoscopy and pelvic pain, hospital das clínicas, faculty of medicine of Ribeirao Preto, university of São Paulo (USP-HCFMRP). We excluded women with a limited understanding of the study and those who refused to participate. Informed patient consent was obtained via a signed document that contained information on the procedures to be performed.
Evaluations based on TCM were performed by two researchers with professional skills and expertise in acupuncture, who used a questionnaire that had been adapted according to Wen [23], Lee [24], Auteroche and Navailh [25], and Pin [26]. Women who fit the inclusion criteria answered questions related to their age, weight, height, marital status, level of education, and number of pregnancies so that the study group could be characterized. During patient evaluation, the following aspects were taken into consideration: present illness; symptomatology; specific locations of MTrPs; start, cause, duration and frequency of symptoms; personal and family history related to pain, breathing performance, sweating occurrence, and sleep quality; reported emotions; and preferences related to color, food, flavors and weather or season. The following aspects were also investigated: thirst, gastrointestinal dysfunction, excreta (feces and urine), menstrual cycle, all five senses, and characteristic pain symptoms related to headache and to musculoskeletal, abdominal, and chest pain. Patients were also evaluated regarding the following: aspect of tongue, skin color, tone of speech, and lips.
Following completion of the questionnaires, all answers regarding each item were carefully analyzed by the researchers, and all reports were considered according to the “yin-yang”, “zang-fu”, and “five elements” theories. The yin-yang theory analyzes the vital energy that flows through the meridians. Zang-fu theory analyzes internal organs through an energy network in relation to numerous factors including anatomical aspect, emotions, mental activities, sensory organs, colors, and flavors [20]. According to zang-fu, organs that are yin in nature absorb and accumulate energy. The viscera correspond to the fu, which is yang in nature and transforms and transmits energy. The five elements theory (wood, fire, earth, metal, and water) states that the elements have an interdependent relationship that generates a state of constant motion and are associated with element factors such as colors, flavors, emotions, feelings, and physiological characteristics. Consequently, the balance of each function depends on the balance of the other functions, which are interconnected within the “yin-yang”, and “zang-fu” theories [19].
The preparation of the database and the spreadsheets was performed by using Microsoft Office Excel. The answers were added to the spreadsheets, and percentages were determined, taking into consideration the meridians with altered energetic behavior in each evaluation. The main meridians with altered energetic behavior were considered to be those with frequencies above 50%; the frequency of yin-yang disharmonies detected in each meridian was also taken into consideration. Based on the answers obtained, with each answer referring to one yin-yang disharmony, and the answers considered when determining the number of alterations in each specific meridian, the main yin-yang disharmonies were those with frequencies above 90%. As to the sample characterization, percentage calculations were also used, except for weight and height when determining the body mass index (BMI) and the body fat (BF) percentages. The statistical analysis was descriptive, and the results were presented as means ± standard deviations (SDs) and frequencies.
We evaluated 50 women between July 2010 and July 2012. The patient’s characteristics are presented in (Table 1). The ages of the patients ranged between 22 years and 56 years. The majority of patients were married (78%), with a elementary school (66%) and one or two children (76%). The average BMI and BF of the patients were 26.86 kg/ cm2 (range: 17.7 — 39.0) and 32.4% (range: 10.7 — 45.7), respectively.
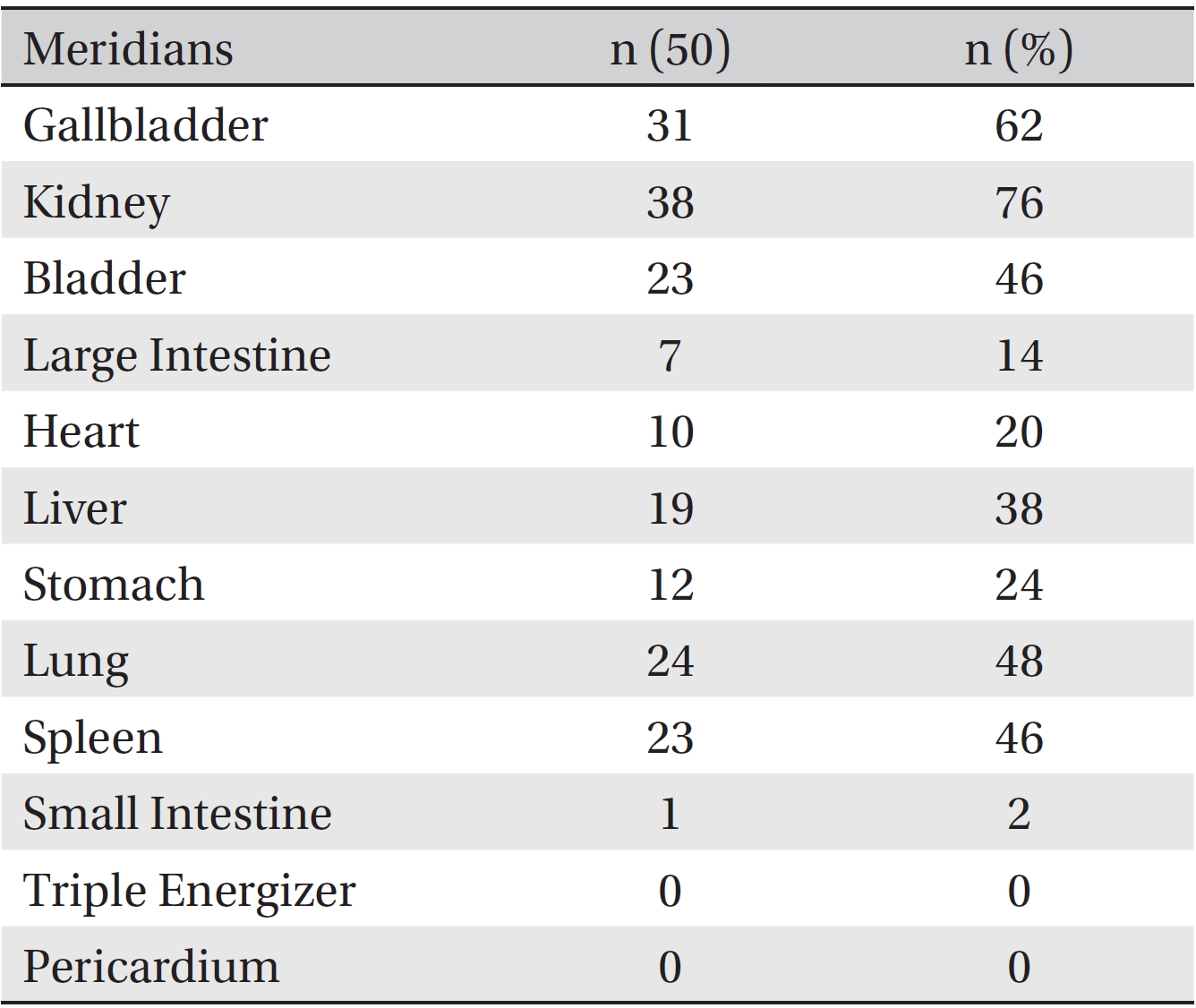
Results of the evaluation based on TCM and innervation corresponding to the pelvic floor are described in (Tables 2,3) From the analysis of each patient’s questionnaire answers, we were able to conclude that, of the 12 zang-fu meridians, only the triple energizer and the pericardium meridians did not show an altered energetic behavior or yin-yang disharmony In contrast, 96% of the women had some kind of major alteration in energy in the kidney meridian, and 98% had major alterations in energy in the gallbladder meridian. The percentage of each energetic alteration in each meridian is presented in (Table 2).
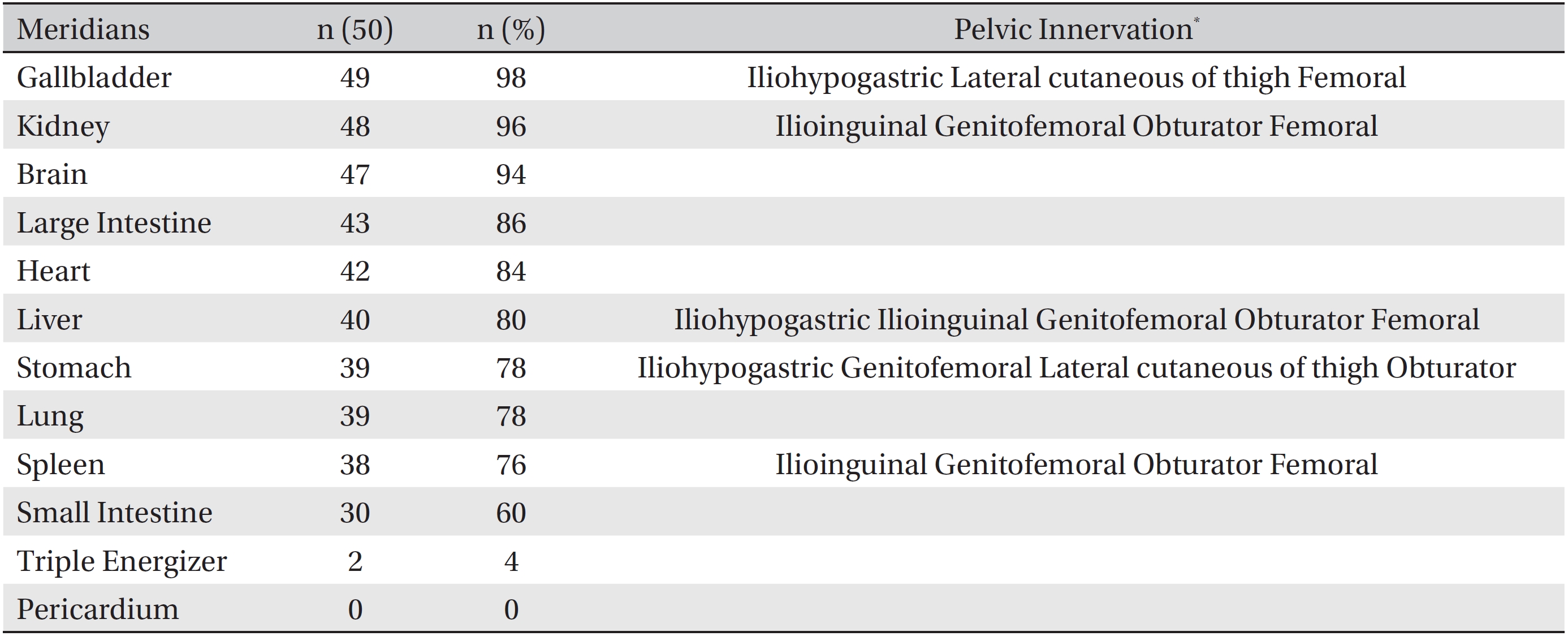
In a second step, we performed percentage calculations corresponding to the major changes found in the meridians, so, we consider only the energy changes above 95% corresponding to the respective zang-fu meridians. This showed that the main yin-yang disharmonies encountered were related to the meridians of the kidney, gallbladder, and bladder. When the sequence of meridians and the frequency of yin-yang disharmony between them were analyzed, the anatomical locations of five of the ten meridians with energetic alterations were clearly similar to the location of the innervation in the pelvic region. The similarities were observed when comparing the trajectories of these meridians with the trajectories of the nerves mentioned. The details of the evaluations based on TCM and on innervation corresponding to the pelvic floor are described in Table 3.
In this study, we used TCM-based evaluations to analyze the Qi behavior of the zang-fu meridians and to verify the yin-yang disharmonies of those meridians in women with a syndrome diagnosis of AMPS. The objective of the study was not to suggest any protocol for the treatment of AMPS. According to this model, diagnosis and treatment are performed through careful assessment based on signs and symptoms while understanding the underlying causes. This is conducted both to relieve surface symptoms and to cure the disease [27].
Our study revealed a greater Qi change and yin-yang disharmony in the gallbladder meridian, a tendon muscle Qi channel with the functions of moving muscles and joints and promoting the body’s defense via blood circulation. Energy dysfunction in this meridian can cause muscle contracture symptoms [28]. According to some authors, the trigger points of anti-phospholipid antibody syndrome can produce muscle spasms, a fact that is in agreement with the results of our study concerning the energetic alteration presented by the gallbladder meridian in women [12, 13].
The kidney meridian showed one of the largest energy changes and yin-yang disharmonies in our study. The chronic pain of internal organs causes a deficiency of this meridian and may produce symptoms such as impotence, sterility, stone formation, oliguria or polyuria, and bloating [28]. Due to this change, the heat propagated in the energy channel (homeostasis) of the spleen meridian becomes deficient, corresponding to the findings of the present study, and can lead to symptoms such as depression, weakness, and fatigue [18]. These symptoms can directly impact the quality of life of these women because they affect emotional and professional aspects of life [2, 7, 8].
By analyzing the evaluation results according to TCM, we identified a similarity between the paths of the five meridians (gall bladder, kidney, spleen, liver, and stomach) and innervation of the pelvic region in support of Gardner
Ruby-Klein
According to Sanchez
At the end of the study, patients were evaluated according to TCM criteria and had obstetrics and gynecology outpatient medical appointments at the USP-HCFMRP for clinical evaluations and further procedures to aid in pain relief. Despite the major role played to the evaluation of diseases through TCM prior to proposing a treatment protocol, few studies have addressed the aspects investigated in the present study, transforming treatment protocols into experiments that depend on the success rate of the selected technique to determine if acupuncture should be implemented as a complementary therapy.
In this study, women diagnosed with CPP secondary to AMPS, who had been subjected to evaluation by using TCM, exhibited changes in Qi, as well as yin-yang disharmonies, in the zang-fu meridians (gall bladder, kidney, and bladder) that were related to major gastrointestinal and urogenital diseases. The paths of some of the principal meridians analyzed were directly related to innervation of the pelvic floor and abdominal region. If an effective treatment is be proposed and a successful outcome is to be achieved, a thorough assessment to establish an individual protocol is necessary.
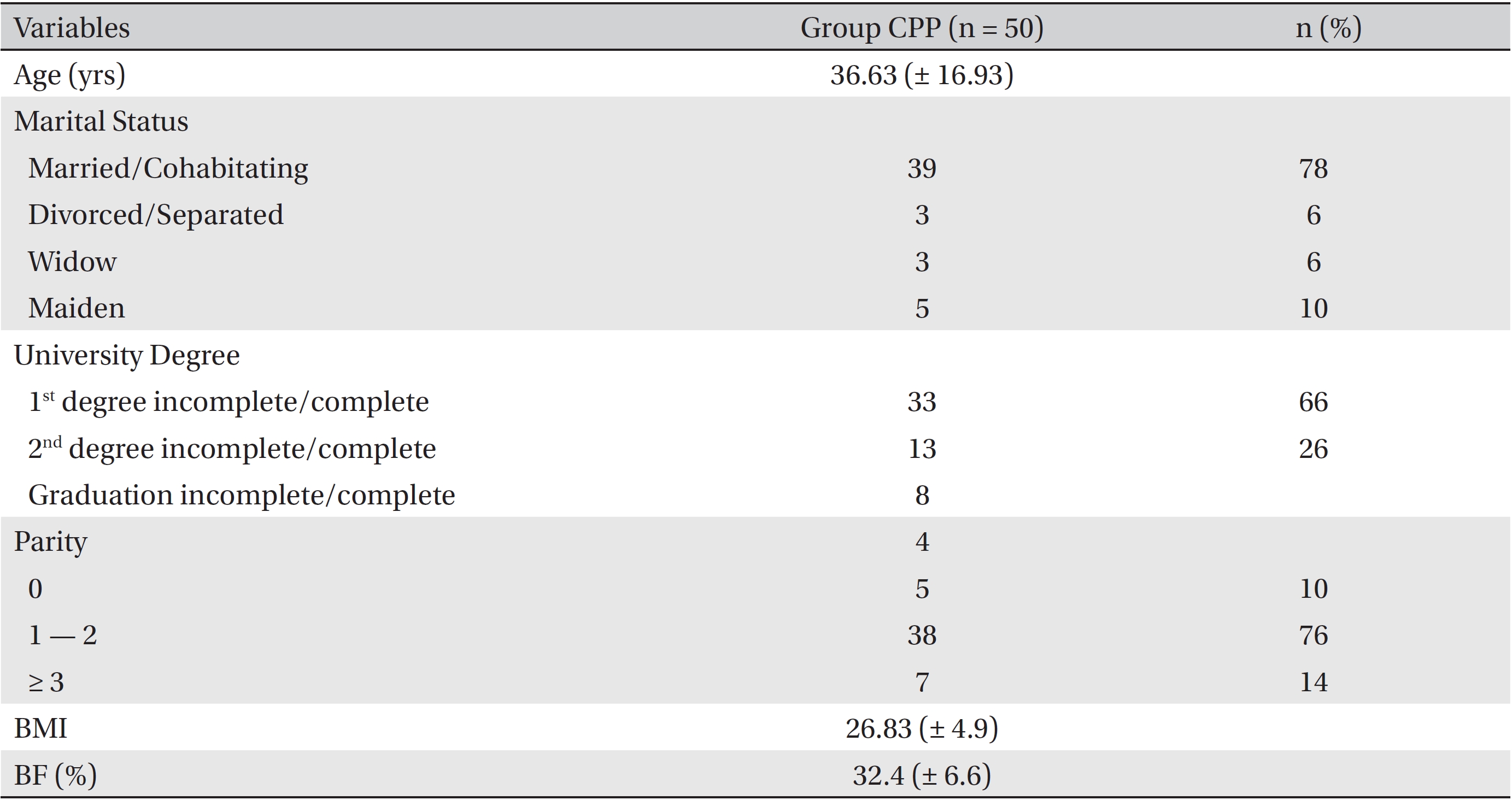
Characteristics of women with abdominal myofascial pain syndrome, as evaluated by traditional Chinese medicine
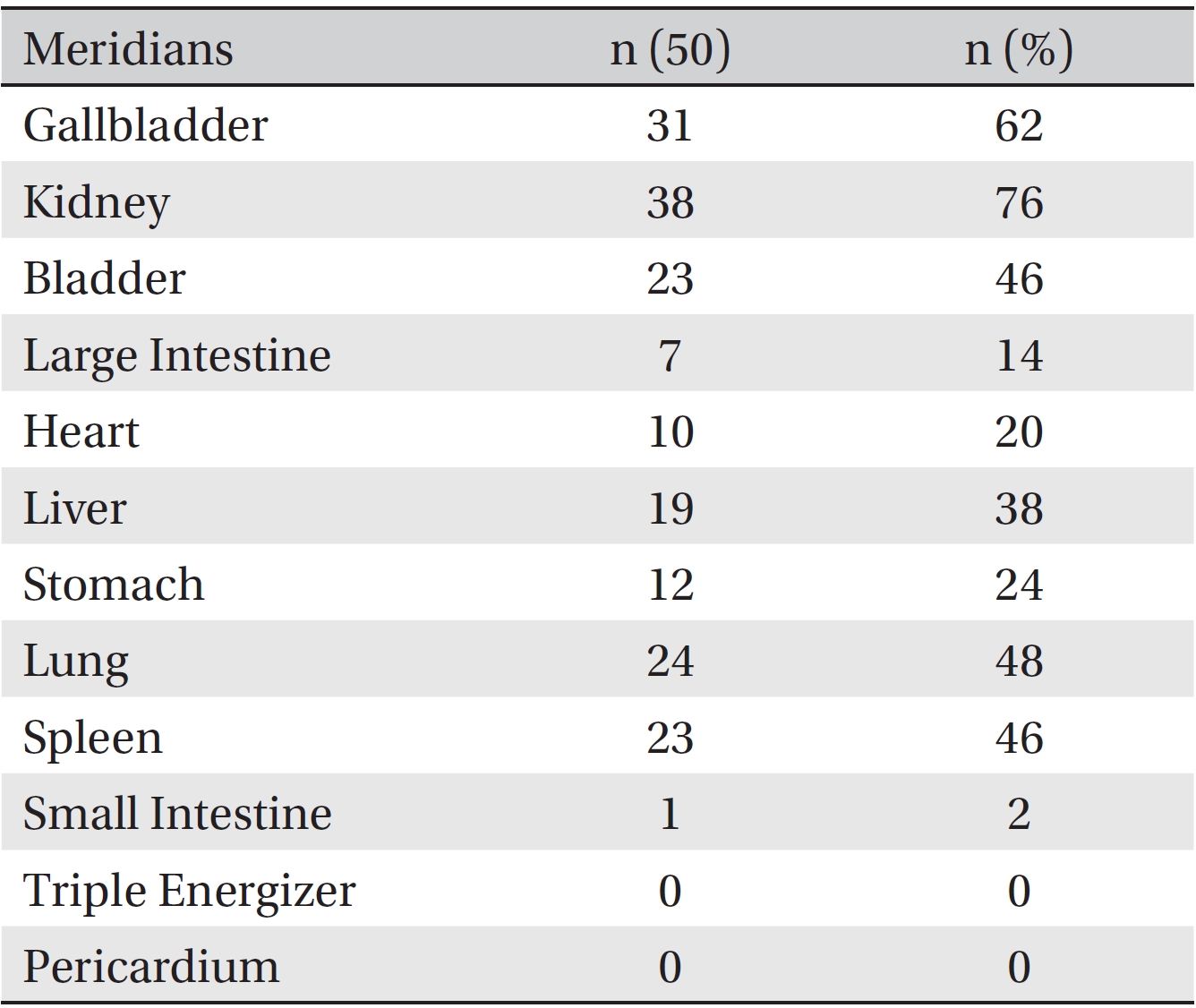
Zang-fu meridians of acupuncture with energetic alterations according to the answers obtained from the traditional Chinese medicine evaluation
[Table. 3] Yin-yang disharmony in acupuncture meridians and corresponding pelvic floor innervation
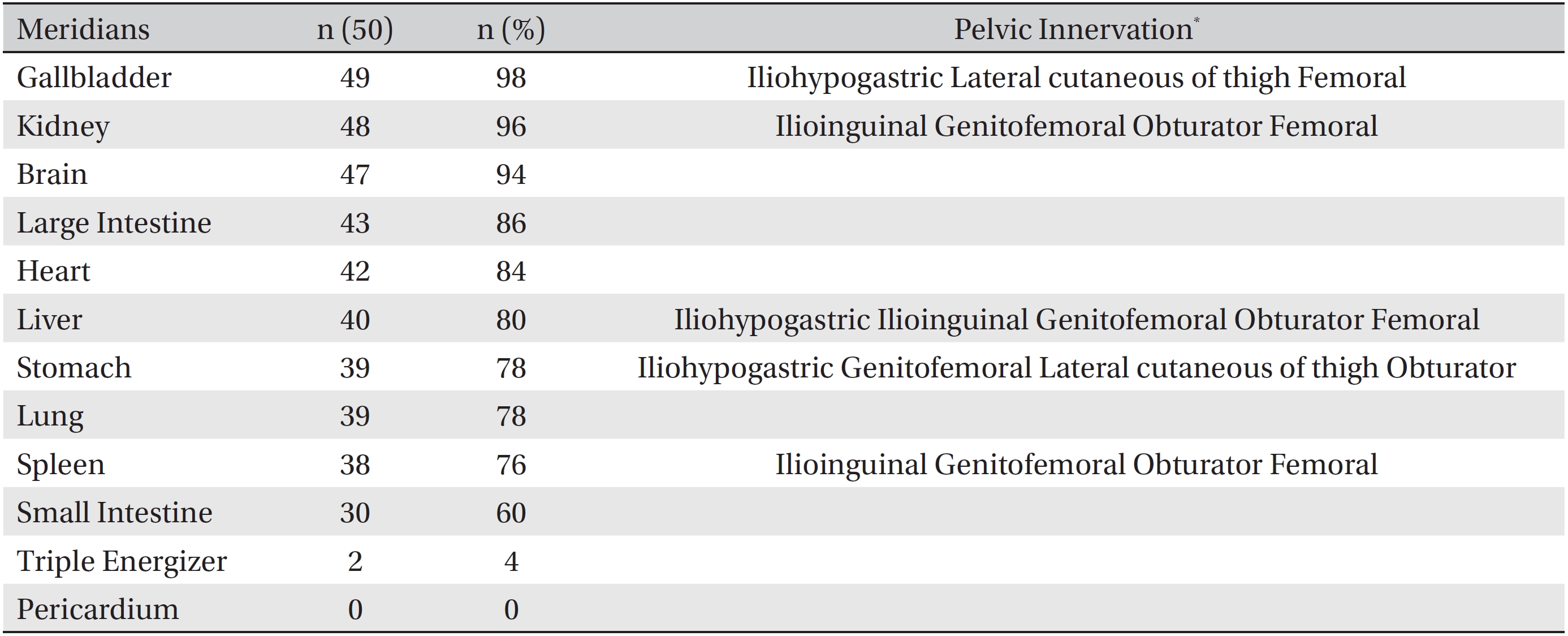
Yin-yang disharmony in acupuncture meridians and corresponding pelvic floor innervation