Dental chair unit (DCU) is the most essential equipment for the dental treatment in dentistry. DCU output water is used for various applications during dental treatment. DCU output water must be clean at the same level as drinking water since patients and dental staff are regularly exposed to water and aerosols generated from the DCU. Many studies demonstrated that DCU output water is frequently contaminated with microorganisms including opportunistic pathogen such as
치과용 유니트(dental chair unit, DCU)는 치과에서 치과치료를 위해 필요한 가장 중요한 장비이다. DCU에는 초음파치석제거기(ultrasonic scaler), 고속 핸드피스(high-speed handpiece), 공기-물사출기(air-water syringe) 등 여러 부속 치과용 기구가 연결되어있다. 대부분의 치과치료에는 이 부속 치과용 기구에서 배출되는 물을 사용한다. 예를 들어, 치아와 부속 치과용 기구 사이 마찰로 발생하는 열을 식히고 시야를 확보하기 위해서, 혹은 소독 후 세척을 위해서 이 물을 사용한다. 환자들은 치과치료 중 부속 치과용 기구에서 배출되는 물에 직접적으로 접촉이 되고, 치과의사, 치과위생사, 치과조무사 등 치과종사자들은 기구에서 발생하는 에어로졸에 항상 노출되어있기 때문에, DCU에서 배출되는 물은 음용수보다 더 높은 수준으로 깨끗해야 한다. 하지만 여러 연구자들의 실험을 통해 DCU에서 배출되는 물이 높은 수준으로 미생물에 오염이 되어있다는 것이 밝혀졌고1-7), 그 중 면역력이 저하된 사람에게 병원성을 보이는 세균들도 검출되었기 때문에, 치과치료 중 사용되는 물로 인해 환자가 세균에 감염될 수 있는 가능성이 제시되어 왔다8-11). 따라서, 미국치과의사협회에서 치과용수 내 세균 수를 밀리리터 당 200 colony forming units (CFU) 이하로 유지할 것을 권고하고 있다12). 오염된 치과용수 사용으로 치과에 방문한 환자들이 세균에 감염되었다는 사례가 국내에는 없지만, 현재 DCU 물과 관련된 논란은 계속되고 있다. DCU 물에 관한 논란과 환자들의 불안감을 줄이고 좀 더 양질의 치과 치료를 제공하기 위해서는 DCU 물의 세균 오염수준을 권고하는 기준치(≤200 CFU/ml)로 유지하는 것이 중요하다. DCU 물의 세균 오염수준을 낮추기 위해서는 DCU 물의 주기적인 관리와 계속적인 소독처리가 필요하다. 현재 DCU 물을 관리하기 위해서 필터와 독립적인 저수통이 설치된 재설계한 DCU를 사용하거나 환자진료 전과 후 수관에서 물을 배출시키거나 화학 소독제로 주기적으로 수관을 청소하는 등 다양한 방법들이 사용되고 있으며, 각각의 방법들마다 그 효능 또한 다양하다. 본 논문의 목적은 DCU 물의 세균 오염 수준과 오염된 DCU 물의 임상적 위험성에 대하여 그 동안 출판된 논문들의 실험 결과를 근거로 하여 설명하고, 세균 오염을 방지하기 위한 여러 가지 관리 방법들을 검토하는 것이다.
1. 치과용 유니트 수계(dental unit water system)의 세균 오염
1) 세균 오염 수준
DCU로 공급되는 물은 일반적으로 독립적인 저수통이나 중앙 급수 시스템으로 제공된다. 치과 병원같이 많은 DCU를 갖춘 일부 대형 치과들은 탱크에 저장한 도시용수를 중앙 급수 시스템이 조절하여 물을 공급하지만, 작은 치과의원의 DCU에는 독립적인 저수통이 연결되어 있어 깨끗하게 처리한 물을 저수통에 담아 둔 후 사용한다13). 대부분 DCU에 공급되는 물은 세균의 함량이 적은 깨끗한 물을 사용한다. 하지만 DCU에서 배출되어 환자의 구강에 접촉되는 물은 높은 수준으로 세균에 오염되어 있는 것으로 보고되고 있다1,2). 터키의 개인치과에서 사용되는 DCU에서 배출되는 물의 오염도를 측정한 Uzel 등3)의 연구에서는 DCU 물이 최대 3.0×105 CFU/ml까지 나타났으며, 영국 개인치과에서 사용되는 DCU의 물 오염도를 조사한 Walker 등4)의 연구에서는 최대 6.4×104 CFU/ml로 나타났다. 또 Barbeau 등5)이 캐나다 치과대학 병원의 DCU를 대상으로 세균 오염도를 조사한 결과, 최대 2.6×105 CFU/ml의 세균 오염도를 보여주었고, 같은 논문에서 새로운 DCU 설치 후 5일 안에 2.0×105 CFU/ml까지 세균에 오염되는 것을 확인하였다. 국내 치과대학 병원의 DCU를 대상으로 오염도를 조사한 Lee 등6)의 연구에서는 최대 3.7×104 CFU/ml의 세균 오염도를 보여주었다. 또한 국내 치과대학 임상 시뮬레이션 실습실에서 학생들의 임상 실습을 위해 사용되는 DCU의 세균 오염도를 조사한 Yoon과 Lee의 연구7)에서는 최대 3.9×104 CFU/ml의 오염도를 나타내면서, 치과 종사자뿐만 아니라 치과대학 학생들도 오염된 DCU의 물에 노출되어 있음을 보여주었다.
2) 오염 세균의 종류
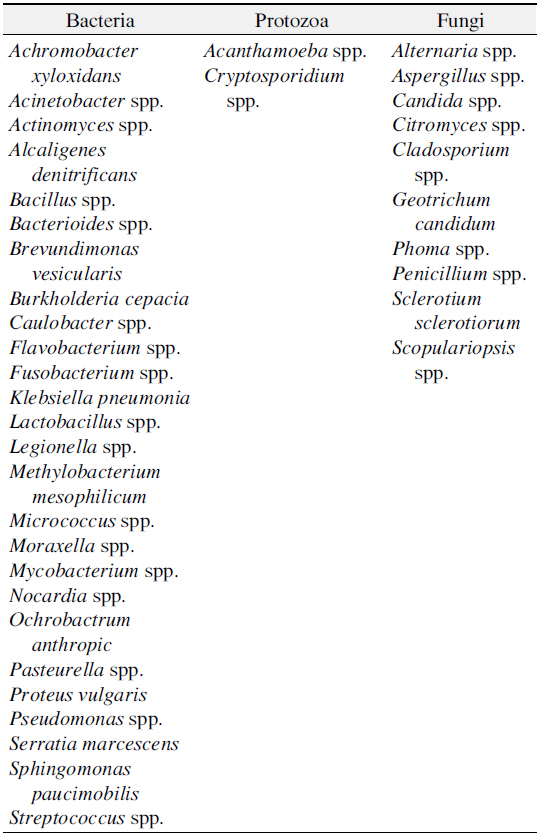
DCU의 물에는 대부분 종속영양성세균(heterotrophic bacteria)을 포함하며 그 중 Yabune 등14)이 연구를 통해
[Table 1.] List of Microorganisms Detected in Water of Dental Unit Water System17,18)
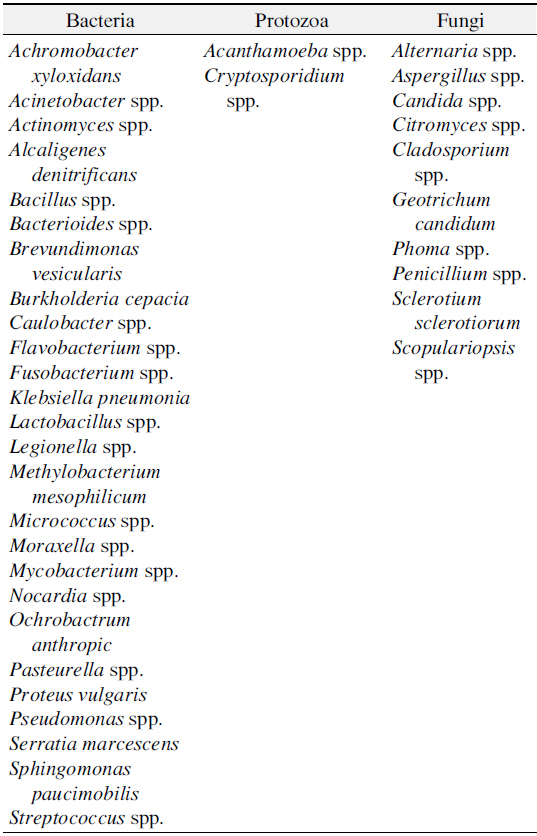
List of Microorganisms Detected in Water of Dental Unit Water System17,18)
1) 수관 바이오필름의 특징
DUWL과 같은 수생 환경에서 흔하게 볼 수 있는 바이오필름은 수관의 내부 표면에 부착하여 성장하는 세균, 곰팡이, 바이러스 등 여러 종으로 이루어진 복잡한 미생물 덩어리이다12,15,22,23). 자유롭게 떠다니는 미생물이 수관의 내부 표면에 부착하며, 이 부착한 미생물은 세포 외 다당류(exopolysaccharide)를 생산하게 된다24-26). 이 세포 외 다당류는 미생물을 수관 표면에 고정시키면서 다른 떠다니는 미생물과 군집을 이루도록 도와준다26-28). 미생물군집이 세포 외 다당류로 인해 이웃하는 미생물 군집과 뭉치면서 바이오필름을 형성하게 된다12,29). 바이오필름을 구성하는 미생물의 세포분열과 새로운 미생물의 추가적 보충을 통해서 바이오필름은 점점 두꺼워진다22,27,29).
Cobb 등30)의 논문에서 수관을 전자현미경으로 확인한 결과, 수관 내면을 바이오필름이 덮고 있으며, 바이오필름이 미생물과 세포 외 기질로 구성되어 있는 것을 보여주었다. 현미경의 고배율에서 구균, 짧고 중간길이의 막대균, 나선형모양의 세균과 같은 다양한 미생물의 형태가 관찰되었다. 또한 타원형의 포자와 같은 구조도 자주 관찰되었으며, 이것은 진균 포자를 나타내는 것으로 추측되었다. 또한 전자현미경을 통해 수관에서 4주동안 성장한 바이오필름의 두께가 30 μm까지 도달하는 것을 확인하였다31).
수관 바이오필름은 DCU에 공급되는 물에 소량으로 존재하는 미생물을 기원으로 하며29), 낮은 유속, 진료시간 외 빈번한 물의 정체, 플라스틱으로 구성된 좁은 내경의 수관은 미생물의 부착과 군집화를 증가시켜 바이오필름을 형성하는 좋은 환경을 제공한다12,32,33). 또한 DUWL은 막 흐름(luminar flow)이라는 특징의 물의 흐름을 가진다12,22,34). 막 흐름이란 수관 내부에 물이 흐를 때, 수관 중심에서 유속이 가장 빠르고 벽으로 갈수록 유속이 느려지는 현상을 말한다. 막 흐름의 현상으로 벽의 물은 표면에 미생물이 부착하고 군집을 이루는 것을 허용하면서 사실상 정체되어있다22,34). 비록 바이오필름이 수관 내부 벽에 고정되어 남아있더라도, 일부 미생물들은 물의 유속으로 인해 바이오필름으로부터 떨어져 나온다. 이렇게 떨어져 나온 미생물들이 환자의 구강 안이나 치과 기구에서 발생하는 에어로졸과 미세 물방울을 통해 환자와 치과종사자의 폐로 들어갈 수 있다12). 따라서 DUWL 바이오필름은 DCU에서 배출되는 물을 지속적으로 오염시키는 미생물의 서식처이자 교차 감염의 잠재적 원천 역할을 할 수 있다10,25,35,36).
2) 수관 튜빙의 재질과 바이오필름
보통 수관 튜빙은 polyurethane 혹은 polyvinylchloride로 이루어져 있다. 이 물질들은 세균이 영양소로 사용할 수 있는 경화제와 첨가제를 포함하고 있기 때문에 바이오필름 형성을 위해 세균이 선호하는 물질이다28). 또한 세균 성장을 억제하기 위해 물에 첨가되는 염소는 polyurethane 튜빙에 의해 흡수되어, 물 속 염소의 농도가 감소하게 된다14). 불소로 내면을 코팅한 튜빙의 세균 부착 억제 효과를 시험한 Yabune 등37)의 연구에서, 일반 polyurethane 튜빙보다 불소로 코팅한 튜빙의 내면에 세균의 초기 부착이 억제되는 것을 보여주었다. 또한 이 불소 코팅 튜빙은 DCU 물 속 염소를 덜 흡수시켜 세균 성장을 방지하기 위해 더 유리할 수 있다고 설명하였다.
3. 기회병원성 세균의 임상적 영향(clinical implications)
1) 기회병원성 세균
DCU에서 배출되는 물에서 검출되는 기회감염성 병원균으로
2) 기회병원성 세균 감염사례
Martin45)의 연구에서, 면역력이 저하된 두 명의 암환자 구강에서
[Table 2.] Cases of Infection by Opportunistic Pathogens in Dental Unit Waterline

Cases of Infection by Opportunistic Pathogens in Dental Unit Waterline
1) 권장수준
미국질병관리본부에서는 일반적인 치과치료에 사용되는 물의 세균 수를 마실 수 있는 물의 수준인 500 CFU/ml 이하로 유지시키고, 수술 시에는 멸균수가 공급되는 독립적 장지를 사용할 것을 권장하고 있다48). 미국치과의사협회에서는 치과치료에 사용하는 물의 세균 수를 200 CFU/ml 이하로 유지시키는 것을 권장하고 있다12). 그 외 치과치료에 사용하는 물을 대상으로 세균 오염도의 기준을 정한 국가가 아직까지는 없으며, 그 외 국가에서는 음용수나 수돗물 내 세균 수에 대한 기준만 제시되어있다. European Union에서는 수돗물(tap water)의 세균 수를 100 CFU/ml 미만으로 유지할 것을 추천한다49). 우리나라는 DCU 물을 대상으로 세균 수의 기준을 따로 정하지는 않았지만, 환경부에서 음용수의 일반 세균 수가 100 CFU/ml을 넘지 않을 것을 제시하고 있다.
2) 비화학적 방법: 물을 미리 배출시키는 방법의 효과
비화학적 방법으로는 DUWS 내에 필터를 설치하는 방법, 독립적인 저수통을 사용하는 방법, 사용 전에 물을 미리 배출시키는 방법 등이 있다. 이 중 DCU 사용 전에 물을 미리 배출시키는 방법이 환자의 치과 치료 전, 중, 후에 수시로할 수 있어 진료실에서 주로 사용된다. 물을 미리 배출시키는 방법의 효과를 확인하는 연구가 많이 진행되어왔고, 그 결과 또한 다양하다. Santiago 등50)의 연구에서 2분 동안 물을 미리 배출시킨 후 세균 오염도가 일부는 기준치 이하로 감소했지만 감소의 폭이 적거나 오염도가 더 높아진 경우도 존재했다. Cobb 등30)의 연구에서는 2분, 3분, 4분 동안 연속적으로 물을 미리 배출시켰을 때, 그 전보다 세균 오염도가 감소하였으며, 물을 미리 배출시키는 시간이 늘어날수록 세균 오염도가 더 감소하는 것을 보여주었다. Mayo 등51)은 초기 1.0×107 CFU/ml로 오염된 DUWS에서 6분 동안 물을 미리 배출시킨 결과 1.3×104 CFU/ml까지 감소됨을 관찰할 수 있었다. 10분과 20분까지 물을 배출시켜 그 효과를 확인한 연구도 존재하며, 20분 동안 물을 배출시켰을 때, 세균의 오염도를 0까지 감소시키는 것을 보여주었다29,33). 대부분의 연구에서 물을 미리 배출시키는 것이 배출하기 전보다 세균의 오염 수준을 낮췄지만 이 중 일부만이 미국치과의사협회의 기준(≤200 CFU/ml)에 적합한 수준으로 도달하였다. 연구 결과에 따르면 환자 치료 전 20분 동안 물을 배출시키는 것이 가장 세균 오염도를 많이 줄일 수 있는 것으로 여겨지지만 이는 치과에서 현실적으로 수행되기 어렵다. 또한 물을 미리 배출시켜서 세균 오염도를 감소시키더라도 바이오필름을 원천적으로 제거하지 못해 보통 30분 후면 재오염이 되므로 비효율적일 수 있다33,50).
3) 화학적 방법
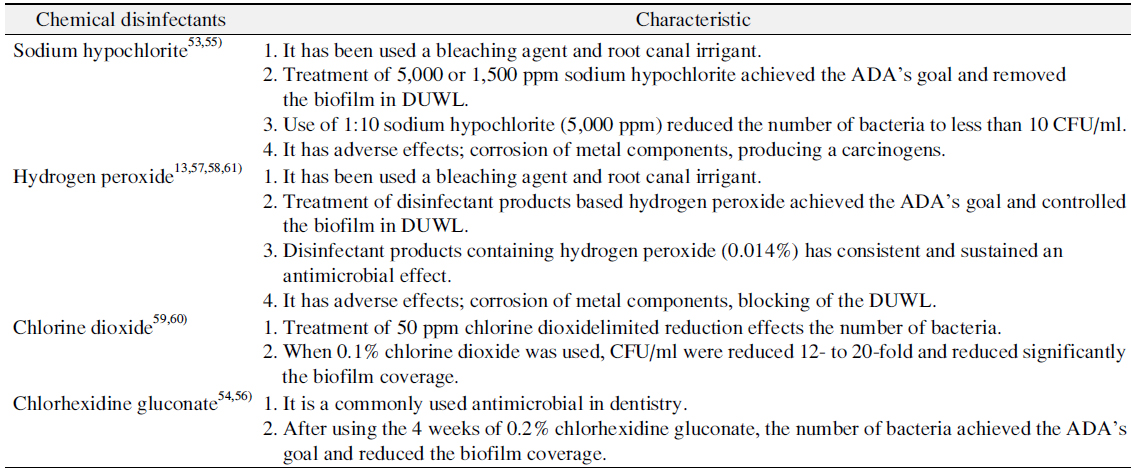
화학적 방법은 항균효과를 보이는 화학물질이 포함된 소독제를 사용하여 DUWL을 소독하는 방법이다. 화학적 방법으로 DUWL을 소독했을 때, 수관 내 세균 오염 수준을 감소시키는 것은 물론 성숙한 바이오필름을 분열시키거나 성장을 억제시키는 것이 보고되었다. DUWS 모델에서 여러 소독방법들의 효과를 비교한 Walker 등52)의 논문에서, 2분동안 물을 미리 배출시킨 후 세균 수의 감소율은 9.1%로 매우 낮았으며, 바이오필름에는 거의 효과를 보이지 않았다. 반면에, 화학소독제품으로 소독한 결과 세균 수를 최소 65%에서 최대 100%까지 감소시켰으며, 바이오필름의 밀도에서 또한 높은 감소율을 보여주었다. 화학소독제를 구성하는 대표적인 화학물질에는 이산화 염소(chlorine dioxide), 차아염소산 나트륨(sodium hypochlorite), 과산화수소(hydrogen peroxide) 등이 있으며(Table 3)13,53-61), 구강양치액(oral antiseptic) 또한 DUWL 소독을 위해 사용되고 있다62). 소독제품들의 소독효과를 비교한 논문들에서 과산화수소나 차아염소산나트륨이 포함된 소독제품이 세균 수의 감소나 바이오필름 감소에 효과적이었고, 6주나 8주 동안 소독효과를 확인했을 때, 200 CFU/ml 이하로 세균 수준을 유지하면서 지속적인 소독효과를 보였다54,56,61). 그러나 효과적인 소독처리의 결과와 함께 부작용도 같이 보고되었다. 과산화수소의 경우, 사용 후 침전물을 형성시켜 수관의 막힘 현상을 보였으며, 금속재질의 치과용 기구에 부식을 일으키고63), 차아염소산나트륨은 금속치과장비의 부식뿐만 아니라, 바이오필름과 같은 유기물질과 반응을 해 발암물질로 분류되는 트리할로메탄을 생성하는 것으로 확인되었다53,57). 소독제품으로 소독 시, 소독제로 하루에 한번 주기적으로 소독한 후 소독제를 낮은 농도로 희석시켜 DCU에 공급되는 물 대신 계속 사용하는 방법이 세균의 오염 수준을 감소시키는 데 효과적임을 제시했다53). 하지만 소독제에 포함된 화학물질이 치아와 수복물질의 결합에 악영향을 줄 수 있다고 보고된 바 있으며64-66), 그러므로 소독효과가 뛰어날 뿐만 아니라 DCU와 구강에 주는 부작용이 적으면서 비용도 낮은 DUWL 소독제품의 추가적 개발이 필요하다(Table 4)28,31,61).
[Table 3.] The Type and Characteristic of Representative Chemical Disinfectants
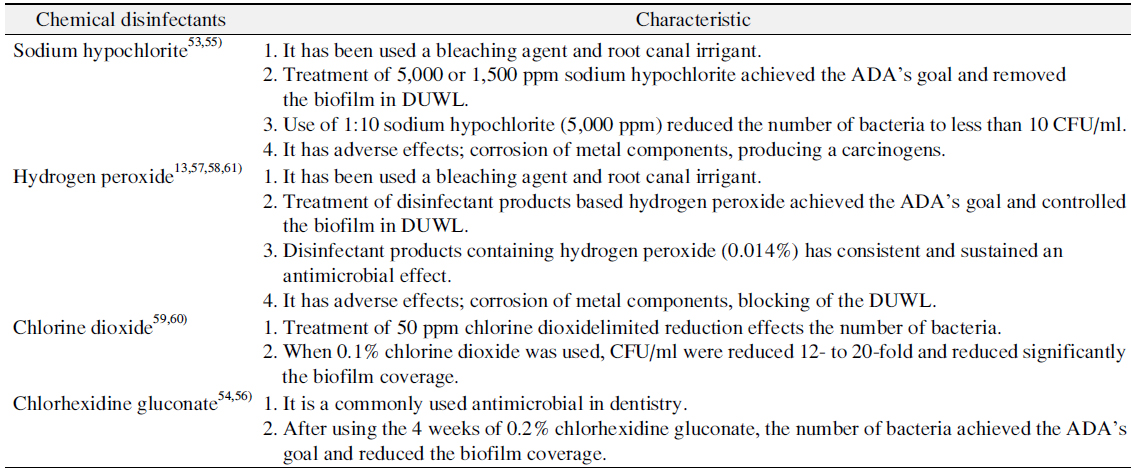
The Type and Characteristic of Representative Chemical Disinfectants
[Table 4.] Disinfection Methods for Dental Unit Water System28,31,61)

Disinfection Methods for Dental Unit Water System28,31,61)
4) 수질 모니터링 방법
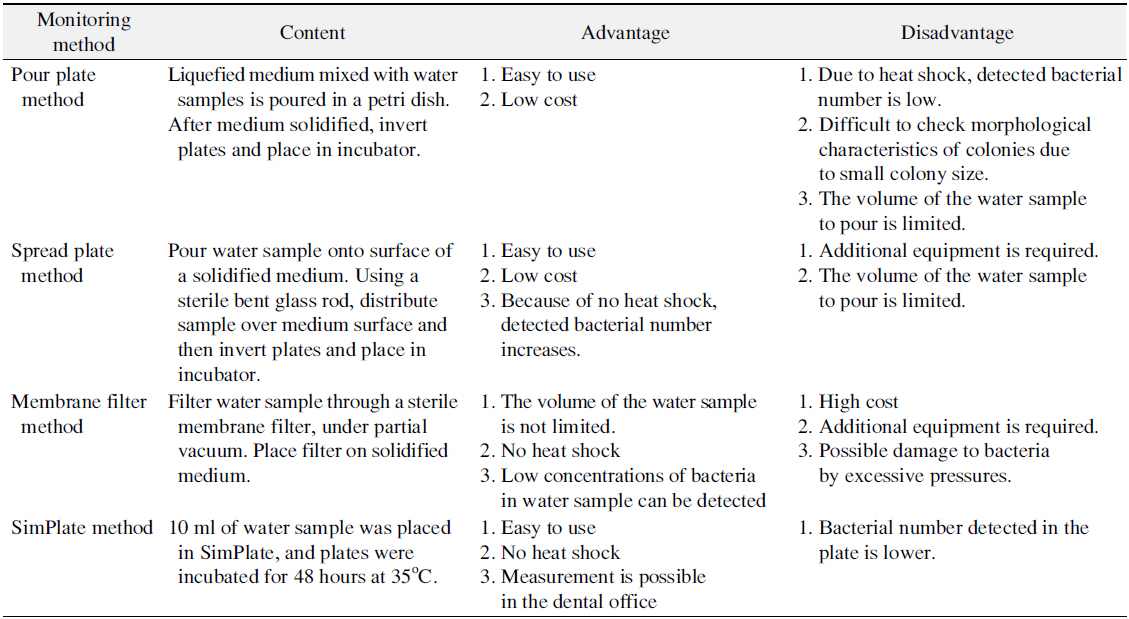
비화학적 방법 또는 화학적 방법으로 소독 후 DUWS의 물 속 세균 수준이 권장하는 수준인지 확인하기 위해 정기적으로 오염 수준을 모니터링하는 것이 좋다. 모니터링하는 방법은 크게 치과 진료실에서 검사할 수 있는 방법과 실험실에 의뢰하여 검사할 수 있는 방법으로 나뉜다. “Standard Methods for the Examination of Water and Wastewater”에서 물 속 종속영양세균의 수준을 모니터링 하는 방법으로 4가지 방법을 소개하고 있다(Table 5)67-69). 이 중 가장 최근에 추가된 SimPlate (IDEXX Laboratories, Westbrook, ME, USA) 방법이 치과 진료실에서 간단하게 검사할 수 있는 방법이지만 이 방법들을 비교한 여러 논문에서 DUWS 물 샘플의 세균을 배양하기에 가장 적합한 방법으로 R2A agar 배지를 사용한 spread plate 방법을 추천한다2,67,69-71).
[Table 5.] Monitoring Methods of Heterotrophic Bacterial Levels in Dental Chair Unit Water67-69)
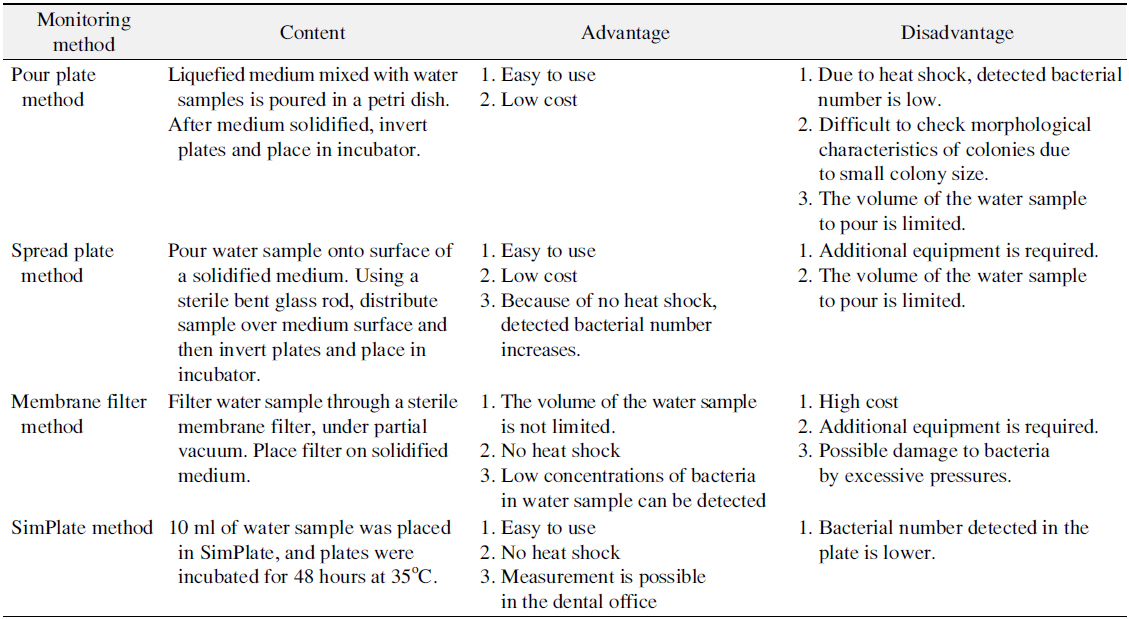
Monitoring Methods of Heterotrophic Bacterial Levels in Dental Chair Unit Water67-69)
미국질병관리본부나 미국치과의사협회에서는 치과용수 내 적합한 세균 오염 수준을 제시하고 있지만, 현재 국내에는 치과용수의 오염을 방지하기 위해 치과수관관리와 관련된 지침이나 세균 오염 기준이 없고, 이를 어겼을 때 받을 수 있는 불이익이나 이 수준을 유지하기 위한 구체적인 수관소독법에 대한 규격화된 관리 지침은 없는 상태이다. 또한 국내에는 치과용수의 오염 실태를 조사한 연구도 부족해 국내 치과용수의 상황에 맞는 지침을 정하기 어려운 상황이다. 비록 치과용수 내에서 검출되는 세균의 병원성이 약하고, 국내에서는 치과용수 내 세균으로 인한 감염이 보고되지 않았지만, 치과용수가 감염의 잠재적 원인이기 때문에 언제든지 치과용수로 인한 감염이 일어날 수도 있으며, 치과치료를 받는 환자들을 안심시킬 수 있는 좋은 치과서비스를 제공하기 위해서는 정책적인 개선과 치과 내 수관 관리 지침이 빠른 시일 내에 시행되어야 할 것으로 생각된다. 치과 관련 학과에서는 치과감염관리에 대해 비중 있게 지도해야 되며, 치과업무에 종사하고 있는 직원들을 대상으로 감염감리에 대한 교육도 철저하게 이루어져야 할 것이다. 하지만 관리를 위한 방법이 다양하고 효과에 대한 정확한 증거가 없어 교육에도 어려움이 따른다. 치과종사자들에게 효율적인 관리방법을 제시하기 위해서는 다양한 관리방법에 대해 많은 연구가 진행되어서 체계적인 관리방법이 개발되어야 할 것이며, 효율적인 감염관리방법을 보편화시킬 필요가 있다고 생각된다. 양질의 치과치료를 제공하기 위해서는 치과종사자의 철저한 수관 관리뿐만 아니라 정책적인 차원의 치과 용수의 오염 기준의 설정이 필요할 것이다.