본 연구는 치면열구전색 하방의 우식이 이차우식에 미치는 영향을 평가하기 위해 DIAGNOdent를 이용하여 소구치 및 대구치 교합면 446부위를 4개의 군으로 분류하였고 상방에 치면열구전색을 시행한 뒤 이차우식을 유발시켜 DIAGNO dent로 재측정하였다. 또한 치과 업무 관련 종사자들을 대상으로 치면열구전색에 대한 인식도 및 실태를 조사하여 다음과 같은 결과를 얻었다.
시진 및 탐침 시 법랑질우식군에서 치면열구전색 후 이차 우식이 가장 높게 나타났으며 초기우식군, 착색군, 건전부위군 순으로 통계적으로 유의한 차이를 보였다(p<0.05). 치면열구전색 전 치아우식증 진단 방법으로는 시진이 가장 높은 비율로 나타났다. 레이저 우식진단기에 대해 56.6%가 모르는 것으로 나타났으며, 91.6%가 보유하지 않은 것으로 나타났다. 치면열구전색 후 이차우식 발생의 원인은 치면열구전색제가 깨져서 하방에 우식이 생긴 경우가 가장 많았다.
이상의 결과를 종합하면, 치면열구전색 하방의 우식이 전색 후 이차우식 유발에 영향을 미치는 것으로 나타났다. 따라서 치면열구전색 후 이차우식을 예방하기 위해서는 열구 내 우식 정도를 정확하게 진단ㆍ평가하는 것이 중요하며, 보다 객관적으로 진단할 수 있는 우식 진단기기의 사용에 대한 교육 및 홍보가 필요할 것으로 생각된다.
Dental caries is one of a main cause of tooth mortality1). The occlusal surface of permanent tooth is very weak on caries, being a first part of decay occurs2,3). Pit and fissure only takes about 13% of occlusal surface but 81% of new decay starts on pit and fissure3-5). According to the dental survey in 2000, 28.3% of 6-year-old children (the eruptive period of the first molar), and more than 50% decay had occurred within 3 years after eruption. And on dental survey in 2005, proportion of fissure caries in immature permanent teeth caries was reported to be 91.8% and 88% in Korea and the United States4).
Sealant has developed and has been used to prevent the decay of pit and fissure6). The sealant makes physical and chemical barriers so the areas can’t be exposed to saliva, food, and oral biofilm7). So it can prevent pit and fissure decay. In 2001, Wendt et al.8) did a cohort research for clinical assessment of sealant on occlusal and buccal pit after 15∼20 years, 65% of the first molar sealant on occlusal and buccal was perfectly maintained, and 22% was maintained partially, but not occurred any secondary caries. Also they reported that sealant effectively prevent dental caries in long-term8). As a result of a sealant stated in the public service in Ireland, the caries was reduced9). And Oulis et al.10) reported sealant could decrease decayed-missing-filled teeth (DMFT) index, Griffin et al.11) proved sealant in permanent teeth reduced dental caries and was effective in caries management. Also, according to the research of Ahn et al.12) on the preventive effect of permanent tooth caries, when water fluoridation is implemented with sealant, it is 4 times higher on the probability of not experiencing caries than water fluoridation played in single. In addition, typically sealant had 75∼97% of the effective caries prevention for a year13,14).
Sealant not only prevent sound fissure, but also used to inhibit the progression of initial caries by closing the upper part of caries lesions6). Furthermore, when applying the sealant to the initial caries reduces microscopic organism and inhibits the ongoing dental tissue destruction15). Simonsen16) reported preventive resin restoration is effective on initial posterior caries or small lesion caries. Heller et al.17) advert sealant was recommended at initial caries because it was effective. Locker et al.18) briefed sealant could obstruct the progression of dental caries lesions on initial tooth caries as well as it could prevent the caries on the sound ones. In 2008, Beauchamp et al.19) recommended sealant for the initial caries lesions that cavity is not formed, based on several clinical evidence about sealant. Sealing on the base and the walls of the fissure caries might be successful as much as sealing sound fissures, said Celiberti and Lussi20). At 2010, Im et al.6) reported it is possible performing sealant on stained or initial caries area, but when performed on a enamel caries area, could detected by exploring, may cause side effects like secondary caries.
Side effects such as secondary caries are associated with the degree of adhesion and leakage between tooth surface and fissure sealant20,21). When the microleakage occurred by fracture of the restoration, microleakage cause discoloration, secondary caries, tooth hypersensitivity, pulpitis20,22). As a result, If you did not apply sealant well on tooth surface, sealant can cause a rather more caries occurrence23).
To date, there are several researches about the effects and leakage of the sealant, but there are few reports whether sealant on initial caries can cause secondary caries. Therefore the purpose of this study is to investigate the influence of the sealant on the secondary caries when the sealant applies on initial caries and analyze the using status and awareness of laser caries diagnostic tool, DIAGNOdent (Kavo, Biberach, Germany), and sealant.
1. Artificial caries degree evaluation
1) Materials
We used the permanent premolar and molar, which was extracted for the purpose of orthodontic treatment, the occlusal surface area of 446 were used as test subjects. And the Ultraseal XT plus (Ultradent, St. Louis, MO, USA) was used as a tooth fissure sealant. DIAGNOdent was used in order to divide the teeth into four groups according to the degree of caries. A buffer solution (0.1 M lactic acid, 13.04 mM CaCl2ㆍ2H2O, 7.49 mM KH2PO4, pH 4.3) was used as a artificial caries lactic acid solution.
2) Group selection and pit and fissure sealant
The occlusal surface of the tooth was performed oral prophylaxis. And tooth occlusal surface 446 areas were divided into four groups according to the degree of discoloration and caries by visual inspection, probe and laser fluorescence caries diagnosis (Table 1).
[Table 1.] Classification of Experimental Groups by DIAGNOdent and the Clinical Examination

Classification of Experimental Groups by DIAGNOdent and the Clinical Examination
3) Artificial demineralization and caries degree evaluation
We induced an artificial dental caries. Put on the teeth one by one into the vial per 0.1 M lactic acid buffer solution by one tooth per 100 ml. And kept on 37℃ thermostat for 6 days. Also, artificial caries induced degree was measured by DIAGNOdent after washing it with distilled water and dry.
2. Pit and fissure sealant awareness and conditions survey
For this study, we produced a questionnaire consisted of 14 questions. And distributed and collected 200 questionnaires on dental clinic in the metropolitan area. Used 166 questionnaires for final analysis excluding no and multiple response questionnaires.
Each item of the questionnaire was carried out frequency analysis. Used one-way ANOVA on evaluating to compare the groups of artificial caries induced degree. And used Dunnett T3 for multiple comparison. Level of significance was set at p<0.05. Data analysis of this study used SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
1. Artificial caries degree evaluation
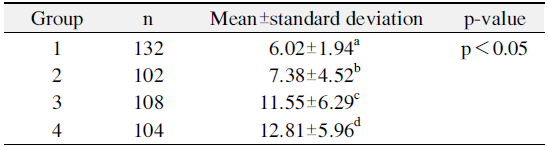
Group 4, clinically detected loss of enamel and indicated DIAGNOdent levels of 21∼29, was the highest as 12.81.
In order of Group 3, Group 2, Group 1, artificial caries level has reduced (p<0.05; Table 2).
[Table 2.] Artificial Secondary Caries Level (n=446)
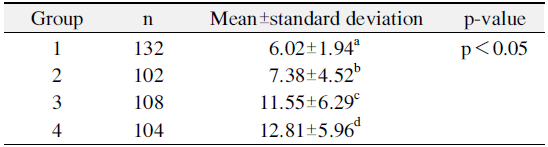
Artificial Secondary Caries Level (n=446)
2. Awareness and usage of sealant
1) Respondents and using status of pit and fissure sealant
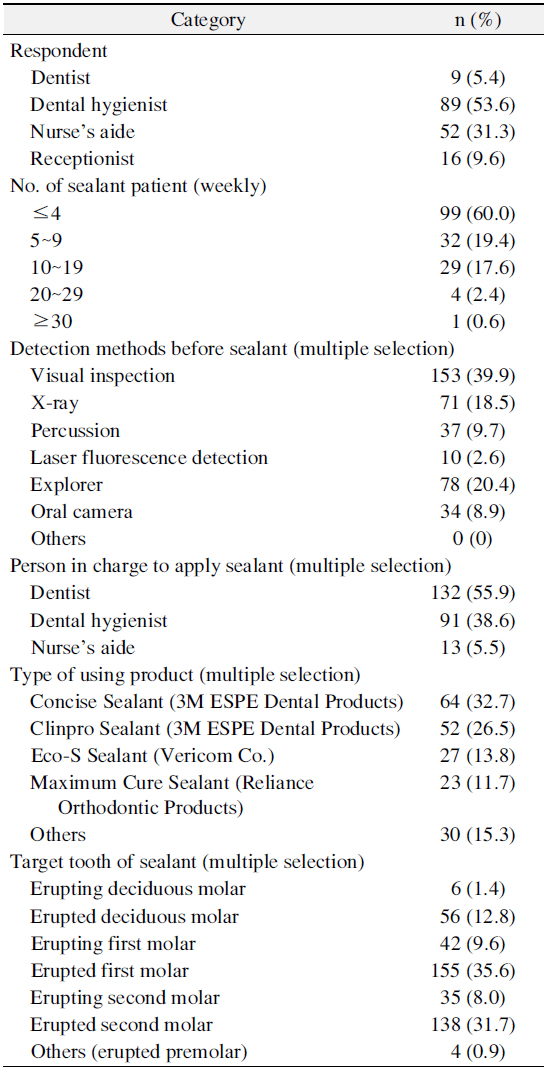
Respondents were consisted of 53.6% dental hygienists, 31.3% nursing assistants, coordinators of 9.6%, 5.4% dentist. The number of patients who had sealant treatment per week was most common at ‘less than four’ as 60% and 5∼9 people, 10∼19 people, 20∼29 people, 30 or more were in the order. The most common diagnostic method before sealant was visual inspection 39.9%, followed by explorer 20.4%, x-ray 18.5%, percussion 9.7%, oral camera 8.9% and laser fluorescence detection 2.6%. Person in charge to apply sealant was 55.9% for ‘dentist’, 38.6% for ‘dental hygienist’, 5.5% for ‘nurse’s aide’. As a type of using sealant, 32.7% for ‘Concise Sealant (3M ESPE Dental Products, St. Paul, MN, USA)’, 26.5% for ‘Clinpro Sealant (3M ESPE Dental Products)’. 15.3% for ‘others’, 13.8% for ‘Eco-S Sealant (Vericom Co., Anyang, Korea)’, 11.7% ‘Maximum Cure Sealant (Reliance Orthodontic Products, Itasca, IL, USA)’. Sealant application areas was highest on ‘erupted first molar’ 35.6%, followed by ‘erupted second molar’ 31.7%, ‘erupted deciduous molar’ 12.8%, ‘erupting first molar’ 9.6%, ‘erupting second molar’ 8.0%, ‘erupting deciduous molar’ 1.4% and ‘others’ 0.9% (Table 3).
[Table 3.] Respondent and Using Status of Pit and Fissure Sealant
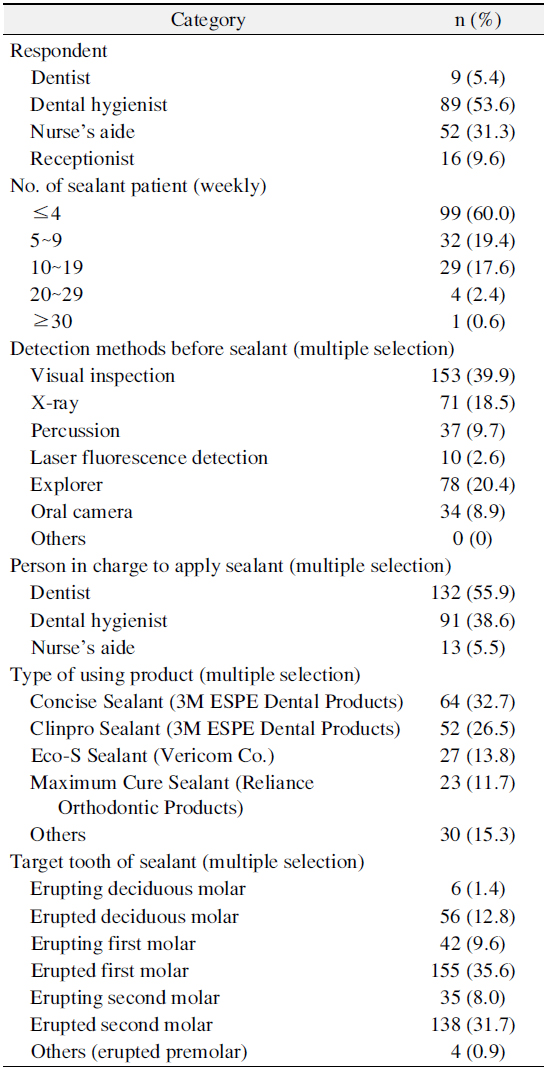
Respondent and Using Status of Pit and Fissure Sealant
2) Using status of laser fluorescence caries device
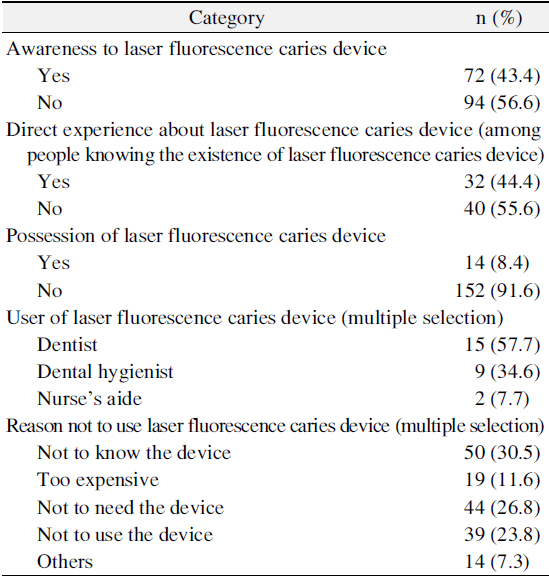
Status recognition about laser fluorescence caries device appeared 56.6% ‘no’ and 43.4% ‘yes’. Among respondents said ‘yes’, when we asked that you had seen the laser fluorescence caries device directly, 55.6% of them said ‘no’ and 44.4% of them said ‘yes’. Answer to ‘Does your dentist possess a laser fluorescence caries device?’ was 91.6% ‘no’, and 8.4% ‘yes’. Also, the answer to ‘Who diagnosis if you had a laser fluorescence caries devices?’ was 57.7% on dentist, 34.6% on dental hygienist, 7.7% on nurse’s aide. Reason of not using the laser fluorescence caries device was ‘didn’t know the device’ 30.5%, ‘didn’t need the device’ 26.8%, ‘didn’t use the device’ 23.8%, ‘too expensive’ 11.6% and ‘others’ 7.3% (Table 4).
[Table 4.] Using Status of Laser Fluorescence Caries Device
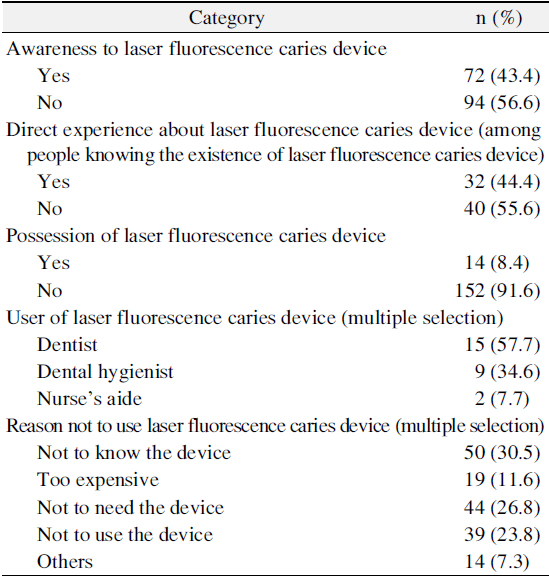
Using Status of Laser Fluorescence Caries Device
3) Occurrence of secondary caries after sealant
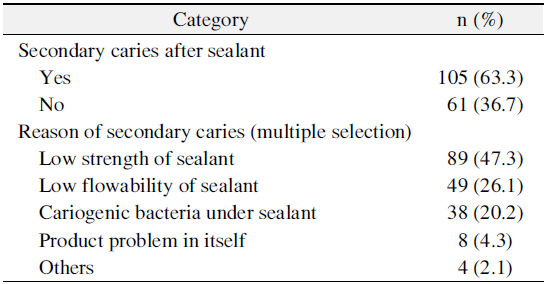
As a answer to a question ‘Whether secondary caries occurs after sealant’, 63.3% said ‘yes’ and 36.7% said ‘no’. Cause of secondary caries was ‘low strength of sealant’ 47.3%, ‘low flowability of sealant’ 26.1%, ‘cariogenic bacteria under sealant’ 20.2%, ‘product problem in itself' 4.3% and ‘others’ 2.1% (Table 5).
[Table 5.] Occurrence of Secondary Caries after Sealant
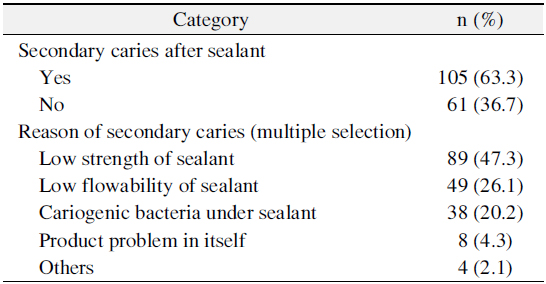
Occurrence of Secondary Caries after Sealant
Diagnosis is very important deciding treatment of initial caries with a filling treatment or sealant24). Diagnostic methods is known as lack of accuracy today, so clinicians carry out sealant even on an initial caries because they couldn’t detect it1). Therefore, in our study, we tried to evaluate the effects on secondary caries when sealant was performed on the upper side of initial caries, using objective criteria of DIAGNOdent.
Fissure is hard to diagnose due to deep and narrow anatomical shape. But it is important to diagnose and evaluate fissure caries correctly and carefully18). As a necessity, various high-tech devices has introduced to diagnose objectively3,5). Among those, DIAGNOdent uses red semiconductor laser light source, measures a total intensity of the fluorescence and displays it with sound and number. It has been put to practical use in clinical caries diagnostic tool25,26). Kim et al.25) reported DIAGNO dent had ability to diagnose quantitatively, depending on the degree caries progression. Lee26) also reported DIAGNO dent could find well-invisible tiny caries and had highly reproducible. In a study of comparison of various diagnostic methods of occlusal carious lesions, Kim et al.27) reported DIAGNOdent is very useful for early detection of occlusal caries. Also, they said it could evaluate more perfectly when used in combination with radiation tests and inspection in case of a progress of dental caries. Kouchaji28) said DIAGNOdent pen is valuable, highly reproducible and accurate diagnostic tool in detecting first molar occlusal surface. Therefore, in our study, the experimental group was classified according to occlusal caries degree using a DIAGNOdent. We excluded a tooth that has already formed a dental caries by limiting DIAGNOdent level under 30 according to other studies which said that tooth, DIAGNOdent level is 35∼40, needs a treatment29,30). Also, our study measured DIAGNOdent level after drying because Lee et al.31) said DIAGNOdent level is more referable when it is dry.
Handelman et al.32) reported as a result of two years’ observation after the sealant has performed above of caries lesion, progression of caries lesions was not shown in clinical and radiological examination. Mertz-Fairhurst et al.33) reported when resin or amalgam filling has been treated above of caries lesion before sealant, it has more clinical success rates and superior maintenance than one with no filling. In our study, results measured by DIAGNOdent were below 0∼13, on all groups, when artificial secondary caries was induced after sealant.
Maintenance of sealant was affected on degree of penetration and leakage. Most of sealant penetrates on fissure about 40∼90%, but most suitable penetrate degree is normally more than 80%. Clinically, there have been a lot of research and effort to increase penetration of sealant, but basically, the degree of penetration receives a lot of influence on anatomical shape34). When Celiberti and Lussi20) compared degree of microleakage and penetration degree of artificial and natural enamel caries lesion sealant group and sound sealant group, degree of microleakage was affected by location of fissure caries lesions and natural caries lesions showed more high microleakage than the sound ones. A penetration of resin gets disturbed because natural caries has a high percentage of organic material. Hevinga et al.35) reported microleakage is higher on decayed fissure because it attached improperly at demineralized enamel. Im et al.6) reported as a result of comparing and evaluating the microleakage and the degree of penetration underwent after sealant, a group of enamel caries was the highest on microleakage among sound, colored, initial caries, and enamel caries groups. Also they said sound group was highest on the degree of penetration in fissure. In present study, enamel caries group (21∼29 level on DIAGNOdent) most commonly caused artificial caries and showed a statistically significant difference in order of initial caries group, colored group, sound group. It is considered that the reason may be low penetration and weak bond strength and microleakage which is most commonly appear after polymerization when tooth fissure caries exist.
Also, in this study, as a results of the questionnaire about diagnostic methods before sealant, visual inspection were the most common and explorer, radiograph, percussion in order. This means that clinicians depend on visual inspection and explorer when they diagnosis. On a question about sealant application areas, ‘erupted first molar’ was highest and followed by ‘erupted second molar’, ‘erupted deciduous molar’ and ‘erupting first molar’. After the tooth erupted into the mouth, the incidence of dental caries was the highest within 1∼2 years after eruption36). Once the sealant was implemented in a child, the age of high caries susceptibility, prevention of dental caries can be further improved36). For this reason, we considered that this result may appear in our study. Also in our survey about laser fluorescence caries device perception, 56.6% said they didn’t know it and among them, 30.5% even didn’t know laser fluorescence caries device existed. Therefore, we could expect that clinicians could perform sealant on initial caries lesion because they failed to detect it by inspection and explorer. So it is considered that education and promotion about the importance and necessity of objective diagnosis is needed.
In this research that whether secondary caries occur after sealant, 63.6% said ‘yes’, and cause of secondary caries was ‘low strength of sealant’ 47.3%. Feigal et al.37) reported it could easily remove when sealant has proceeded without using rubber dam. Also, Park et al.38) said shear bond strength significantly decreased in case of contamination in saliva. It is impossible to block any moisture or saliva completely on dental treatment38). So we considered that using rubber dam is a necessary part for successful sealant.
Taken the results of this study all together, caries under sealant expected to affect secondary caries in afterwards and it is important to need publicity about the use and necessity of an objective fluorescence device.
This study was designed to know how caries under sealant affects on secondary caries. After dividing 446 areas of occlusal surfaces into four groups, we performed pit and fissure sealant on the upper side of fissure, caused secondary caries and used DIAGNOdent to measure degree.
In addition, as a result of the investigation for recognition and using status of pit and fissure sealant, the following results were obtained. First, when visual inspection and explorer had done, secondary caries after sealant on ‘enamel caries’ group was the highest, followed by ‘initial caries’, ‘colored’ and ‘sound’ group. And it was showed a statistically significant difference (p<0.05). Second, visual inspection showed the highest rates on diagnostic methods before sealant. Third, 56.6% didn’t know about laser fluorescence caries device and 91.6% of them didn’t have it. Forth, cause of secondary caries was ‘low strength of sealant’.
Taken all the above results, caries under sealant expected to affect secondary caries in afterwards. So it is important to diagnose and evaluate caries perfectly on preventing secondary caries, also it is believed to need publicity about the use and necessity of an objective fluorescence device.