To describe the progress and influencing factors of Hwa-byung.
Data were collected from semi-structured interviews. The progress of and recovery from Hwa-byung were examined using the collected experiences of eight middle-aged women who suffered from Hwa-byung. For analysis of the data collected, a Consensual Qualitative Research (CQR) methodology was used.
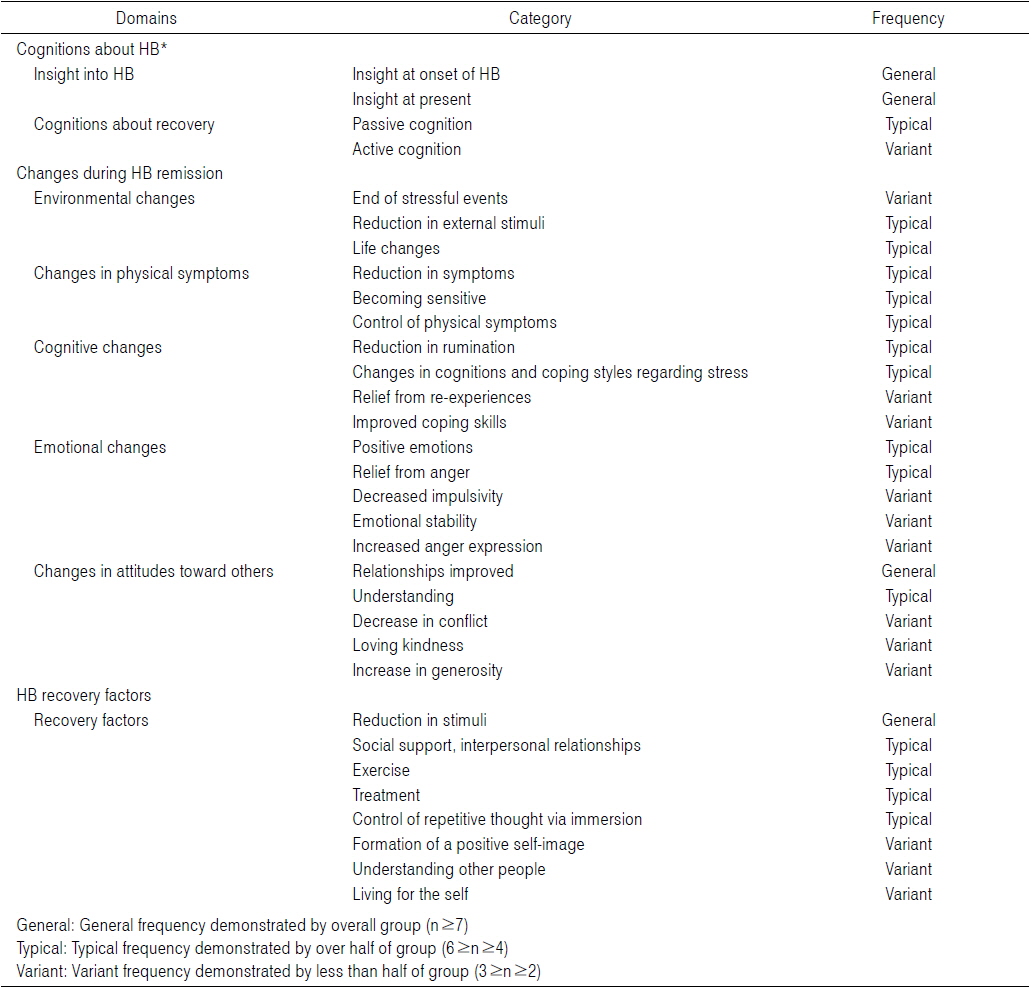
Of the eight participants who thought they had Hwa-byung, six were actually Hwa-byung patients and two were non-Hwa-byung patients. Four years later, four of the six Hwa-byung patients recovered, while the Hwa-byung of one patient persisted, and the remaining patient had circular Hwa-byung. Over time, the symptoms of Hwa-byung declined substantially. However, the patients recognized that their disease continuously persisted. Moreover, they thought their symptoms had worsened. Many types of changes were observed during the recovery period, including environmental, physical, cognitive, and emotional changes, as well as changes in attitudes toward others. Recovery factors included the reduction of stimuli, social support, exercise, treatment, control of rumination, and some cognitive changes.
To recover from Hwa-byung, it is necessary for patients to experience changes in environment, cognition, and emotion, and to employ self-management in everyday life.
Hwa-byung (HB) is a disorder characterized by physical symptoms caused by anger, depression, and Han1). A suppressed form of anger and depression caused by stress transforms into Hwa. In the DSM-IV, the American Psychiatric Association defines this phenomenon as a culture-related anger syndrome generated from sociocultural characteristics distinctive to Korea2).
The prevalence rate of HB is between 4.2 and 13.1%; most patients are middle-aged females3-5). HB is thought to relate to the male dominated family structure in Korea, which requires female members to passively endure suffering. An epidemiological study on HB patients has indicated the main cause is stress induced by husbands and parents-in-law. This provides a reasonable explanation for why middle-aged females form the majority of the patient group3). These conventional studies clearly exemplify the existence of a correlation between HB and gender, demonstrating that there is a clear connection between female psychology and HB in Korea.
However, conventional studies HB mostly concentrate on the concept, psychological characteristics, diagnosis, and treatment of HB, while only a handful of studies consider a specific approach to the disorder in terms of its sequential progress and specific experience. Epidemiological studies have been carried out in order to investigate the pathophysiological characteristics of HB, and these studies have revealed certain differences existing between groups of patients whose symptoms worsen to HB and those that tend to recover from their condition3). However, there are few studies on patients’ internal changes and the factors affecting their recovery. Thus, this study aims to investigate the progressive process, as well as factors affecting recovery based on patients’ experiences by conducting a qualitative study with middle-aged women, who make up the majority of HB patients.
This study utilized Consensual Qualitative Research (CQR)6), a system used for researching internal data through an inductive and exploratory process, based on a small amount of interview data in order to determine the prognosis and factors influencing recovery of HB patients.
The study was carried out with patients who visited us thinking that they had HB. Among those who participated sufficiently to receive an adequate decision on their progress and recovery, patients who agreed to participate in a qualitative interview were selected to be the study participants.
A semi-structured questionnaire was devised based on relevant documents and theory. The questionnaire was then revised by two HB specialists. Based on this questionnaire, standardized questions and items were constructed. The questionnaire included causes, pathology, periodical changes, progression changes, and factors related to recovery, through discussion using an open question format.
Interviews were conducted by researchers with clinical experience. The purpose of the study was explained extensively before getting participants’ consent. Researcher interviewed participants one by one about 3~40 minutes at independent room. Interview data were gathered based on a semi-structured questionnaire, while the entire process was recorded for further analysis. The collected data were categorized and encoded based on similarities by researchers with experience about HB and qualitative research. Certain domains were set for defining main concepts, while subcategories were formed to develop a theory of the HB recovery process and its factors.
1. Characteristics of participants (
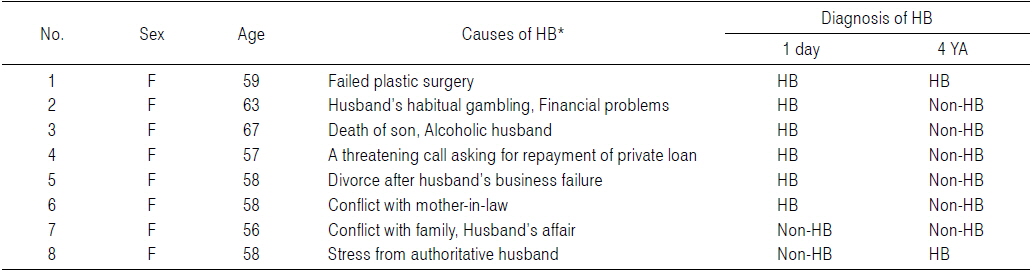
[Table 1.] Hwa-byung Causes and Diagnosis
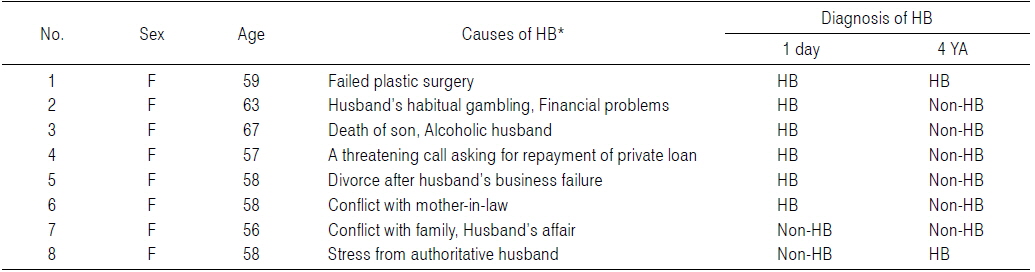
Hwa-byung Causes and Diagnosis
Patients who participated in this study either recognized that they had HB themselves, or HB were told by people in their environment that they had HB. A total of eight people agreed to participate in the qualitative study. Six of them were homemakers and two had vocations. Causes for HB were reported to be the participants’ husbands in five cases, parents-in-law in one case, debt in one case and a failed plastic surgery for the remaining patient. Their average age was 59.5±3.43 years.
[Table 2.] Description of Domains and Categories
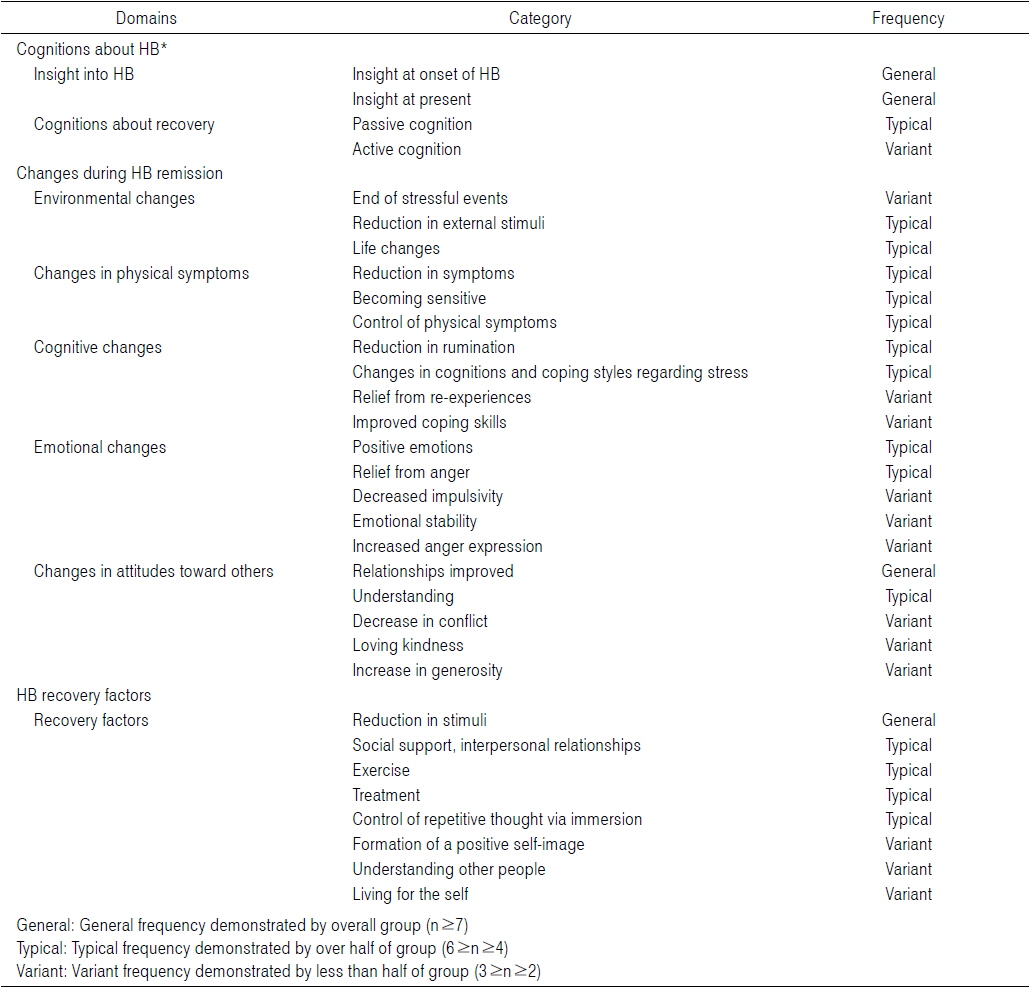
Description of Domains and Categories
Perception in this context refers to whether the patients recognize and understand their own disease and whether they know about its cause and curability. Most patients were well aware that they were suffering from a disorder called HB, and clearly recognized that they had the disease even when their symptoms got better, based on their stress reactions and several other symptoms. Most of them also demonstrated a passive point of view on the matter, as they thought that making changes in external factors was the only way of curing HB.
1) Insight into HB
Insight into HB refers to whether the patients were aware that they had HB during their first visit and their perceptions four years later.
(1) Insight into disease at the point of onset
Seven of the patients indicated that they knew they had HB before being informed of their Structured Clinical interview for the DSM-IV Diagnosis (SCID) results. Two patients that were not diagnosed as having HB according to the SCID also reported that they thought they had HB based on their symptoms and psychological condition. After diagnosis, those patients did not demonstrate any change in their insight into HB, as they had reported that “their symptoms are still minor” and the “others’ HB is more severe.”. One participant that did not have insight into HB said that she came to realize that she had HB while participating in the stress interview and answering questionnaires: “I knew that I had HB as I couldn’t help myself from having a sudden surge of anger.”
(2) Current insight into the disease
All eight participants replied that they thought they presently had HB, while six of them were diagnosed as not having HB anymore due to the low number and severity of major symptoms. However, the participants perceived what they experienced when stressed as HB, and believed that they were still HB patients.
“My symptoms have diminished...but I get immersed in those thoughts as I get a surge of anger and a rising heartbeat...getting into this emotional state makes me feel that I still have HB.”
2) Insight into HB recovery
Most participants responded that recovering from HB is very possible, but had different ideas on the recovery itself. While most patients perceived the situation from a passive point of view, considering external factors of recovery, only two participants replied that they would actively pursue changes, as they believed recovery could be achieved from internal factors.
(1) Passive insight on recovery
Passive insight into recovery refers to the belief that there should be external changes in order for recovery to take place. Most participants in this study were found to hold this point of view, believing that they would not recover unless the causal factors were removed from their lives.
“⋯It seems to get better when my husband is good to me but HB comes right back when he gets on my nerves again. I think I would get better if my husband stopped irritating me”
(2) Active insight into recovery
Active insight into recovery refers to a way of thinking found in some participants that they believe changes in themselves and having determination can cause recovery from HB.
“I believe that all things depend on things I do. I think controlling urges of anger would make my condition better.”
HB actively changes in relation to external stimulation and stress. Changes in the HB recovery period include aspects categorized based on both external and internal changes that participants experienced.
1) Changes in environment
External stimuli refer to those stimuli that participants reported to have a causative effect on their HB.
(1) Termination of stress event
Termination of stress event refers to a situation where the event considered by the participants as causing HB has ceased to exist. As a result, stress and emotional stimuli are reduced. Participants responded that the termination of a certain stress event helped them to gradually recover from their state, as there was no more stimulation.
“As I didn’t have to see him anymore after the divorce, it got a lot more comfortable.”
(2) Decreased external stimuli
This category was based on patients’ responding that they experienced a reduced degree of symptoms after distancing themselves from and reducing the length of exposure to external stimuli.
“It was immensely hard for me when my husband was at home after retiring from his work...as he was at home after retirement, there were a lot more things to have conflicts over...now that he is out at work it got a bit better...it feels like I can at least breathe now.”
(3) Changes in lifestyle
Patients felt that changes in daily life had a correlation with their recovery apart from anything related to the cause of HB. There have been reports from patients that events such as their children’s marriages, births of grandchildren, acquirement of a new vocation, and retirement from work facilitated a new range of emotions, leading them to experience an alleviation from HB.
“It got a lot better when I was seeing my daughter-in-law as I was preparing for my son’s marriage.”
2) Changes in physical symptoms
This refers to changes in physical states, such as hot flushes, chest pressure or pain, heart palpitations, and feeling surges that patients considered symptoms of HB.
(1) Decrease in symptoms
All participants concluded that their HB had diminished over time according to their symptoms. They reported decreases in stress reactions and physical symptoms in everyday life, which led them to believe that their HB had alleviated.
“...It’s all the same that I get stressed, but back then I used to experience involuntary sighing, increased heartbeat, and hot flashes, but these days, I have far less of those. It makes me feel that I’m slowly recovering from it.”
(2) Hypersensitivity to stimulation
Hypersensitivity to stimulation means to have HB symptoms even with minimal exposure to stimuli. Even when feeling better off in terms of symptom severity and not experiencing symptoms according to the SCID, participants have reported experiencing symptoms from a low amount of stimulation and that their bodies became more vulnerable and sensitive to stress and stimulation.
“...Sometimes I feel perfectly okay⋯ but it gets harder from time to time as I get so sensitive to such little things with my heart pumping and the whole body aching.”
(3) Regulation of physical symptoms
This refers to participants having the experience of being able to control certain HB symptoms by their own will. Those participants have reported that by implementing measures, such as diet therapy and exercise, they have been able to regulate their symptoms, resulting in an overall decrease in symptoms.
“At the point of recovery I began to go hiking. Before then, I used to get a strong feeling of stuffiness, but after I started going hiking an hour a day, my breathing got a lot better and I started to feel much relieved. I still go hiking when things become stifling.”
3) Cognitive changes
Cognitive changes denote transitions in cognitive factors, such as thoughts, and the manner of reacting to stress at the point of recovery. Cognitive changes were further subcategorized into decrease in rumination, alteration in stress recognition, diminished re-experiencing of past events, and improved ability to cope with stress.
(1) Diminished rumination
Diminished rumination refers to a patient’s ability to avoid counter-productive ruminative thinking and repeated immersion in causal or stressful events related to HB. Participants reported a reduced number of ruminations as they started concentrating on other activities, exercising, and having conversations.
“Before then, I just started contemplating when things happen, thinking over and over about what I got mad at. But now, I try not to think about those things so I choose to think about or participate in other things.”
(2) Alteration in stress recognition and method of reaction
This is a changed ability to perceive stress. The majority of participants have changed in their response to stress, from avoiding or reacting in a counter-productive way to being able to cope with the situation.
“I’m still becoming stressed, but now I think that everyone else gets stressed and has to accept the situation as it is, when I used to get unbearably angry before.”
(3) Diminished re-experiencing of past events
It was very common for participants with HB to continuously suffer from thoughts about and re-experiences of past events and incidents. Because such re-experiencing can be triggered by a minimal amount of stimulation and intensifies HB symptoms or causes it to recur, its decline is thought to correlate with HB recovery.
“During holidays, I keep remembering the stress I had before and those thoughts keep lingering in my head. Then I get stuck in this maze of mine and get sick again. But now, I don’t want to do that anymore. I think about those things far less during holidays and even when I do, it’s much less painful now.”
(4) Improvement in stress coping capability
Improvement in stress coping capability refers to being able to handle and accept stressful events in everyday life, other than those that have caused HB, more skillfully than in the past. Study participants responded that while having HB, they got over other types of stress relatively easily, considering those events as being aspects of the transient agony of everyday life or minor events.
“It all seems so futile to me now. Seeing it as something passing, not a big deal⋯after a while it would all be nothing.”
4) Emotional changes
This category is based on the emotional changes that participants went through at the point of recovery. The most common of these were a decrease in negative emotions, such as anger and resentment, an increase in positive emotions, and an overall stabilization of emotions. Some participants have also reported having experienced an increase in anger expression.
(1) Increase in positive emotion
As patients go through the recovery period, the percentage of positive feelings, such as joy, delight, hope, and relief, tends to increase steadily, affecting their overall emotional state. Most participants reported that they experienced joyful emotions and delight while recovering from HB.
“As I started traveling around after closing my shop, I began to realize that there was so much fun in the world. Everything was so much fun and enjoyable...this feeling of emancipation was the best. Then HB got a lot better.”
(2) Diminished anger
Diminished anger refers to a decrease in anger within the patients as well as in its outward expression.
“I used to get angry often as I was hot tempered, but, as I started trying to lay down everything and to restrain myself, I got angry a lot less than before. Once I was able to hold things back, my anger started to dwindle.”
(3) Decrease in impulsiveness
Impulsiveness combined with anger in HB patients tends to be expressed as aggression, impulsive actions, and internal impulsiveness. Participants reported that characteristics they used to have, such as a hot temper and impulsive expressions of anger, had diminished.
“Sometimes I get this surge of anger and resentment. When that happens, I really want to quit everything and just start fighting and get sick...now, these surges have diminished.”
(4) Emotional stability
It is not uncommon for HB patients to experience a high level of emotional tension and anxiety because of ongoing stress or conflicts. Emotional stability refers to the diminished anxiety and a state of constant emotional stability and tranquility that patients experience as their HB subsides.
“I started to be able to get relaxed. This helped me attain stability in my mind and control a feeling of anger.”
(5) Increase in anger expression
As patients recover from HB, some of them reported a contradictory increase in the expression of anger. These participants thought that their way of keeping that anger to themselves has led to a worsening of HB. Hence, they reported an increased number of incidents where they expressed their anger while actually recovering from HB.
“⋯in past days, I just kept everything to myself when I was told of these things, but now I shout back at them. Keeping things to myself eventually caused me to have HB. I keep thinking that I should restrain myself, but now I can’t and that’s when I start bursting into rage...I’m fine usually, but these things happen when I get edgy from time to time.”
5) Changes in the way patients treat others
This category was formed based on changes in participants’ relationships with their families, friends, and people around them. It is common for HB patients to attribute the cause of the disease to people around them and to have conflict with others as they experience anger, resentment, a victim mentality, and repulsiveness. A series of internal changes the patients go through as they recover from HB present in their relationships with others, leading to changes in the relationships.
(1) Improvement in relationships
Improvement in relationships refers to the deepening of personal relationships that patients experience as they resolve certain conflicts with others and feel that they are getting along with others better than before. All patients reported that their relationships with other people had improved as they started recovering from HB.
(2) Increase in understanding
When patients’ ability to understand others grows, it tends to affect their recovery from HB as they begin to control their emotions in conflict situations. Most participants responded that their ability to understand, as well as the depth of that understanding, had increased as they began recovering from HB. Some participants also reported that this increase in understanding ultimately caused cognitive changes and decreased anger.
“As I started doing these sessions and learning from them, there were certain things that I happened to realize about other people’s minds...as I start to understand others, it had a remedial effect on me as well...I used to just hate these people, but I can accept these things more freely now.”
(3) Decrease in number of quarrels
Quarrels are a visible form of conflict between people. Participants responded that the number of quarrels they had with others diminished as they recovered from HB.
“I used to just start fighting with others when they say things, but fewer and fewer of those quarrels are happening these days. People around me are also saying that I get along with others better these days.”
(4) Formation of affection
Affection here refers to feelings of love and benevolence. It means that patients start feeling affection toward others as they start recovering from HB. Some participants have reported having greater empathy toward others and feelings of warm-heartedness, indicating the formation of affection.
“Thinking of that person, I feel sorry for him and sometimes am full of pity. It gets to me that I should be good to him as I know that he also would be having a very hard time⋯”
(5) Acceptance
As the range of patients’ acceptance widened, patients became more relaxed overall. Patients reported that they were more tolerant in relationships and became more hospitable to situations they encountered.
“As I put myself down and tried to accept that person as he is, I actually was able to accept him.”
4. Factors Relating to HB Recovery
While recovering from HB, participants experienced various internal and external changes. Factors that have a direct correlation with HB recovery and remission were organized into this category HB. Participants 1 to 7 had more than one incident of recovering from HB. The eighth participant, on the other hand, kept trying to reduce her HB symptoms and saw visible changes, although she did not perfectly fit the HB diagnostic criteria. Therefore, an examination was conducted on factors that were thought to be effective for HB recovery and actions that patients attempted on their own.
The factors relating to HB recovery were as follows: decrease in stimulation, personal relations and social support, exercise, treatment, inhibiting repetitive thoughts via immersion, formation of a positive selfimage, understanding other people, and living for oneself.
(1) Decrease in stimulation
All patients responded that a reduction in stress-inducing stimuli had helped them recover from HB and that this was the most important factor. Participants responded that HB symptoms alleviated as their stress levels declined with the decline in external stimuli.
“(Recalling the time she was recovering) After paying back all of my private loan, I could lay things down and the hardship got a lot better as there were no more calls urging payback.”
(2) Personal relations and social support
Most participants responded that social support, stability, and joyful experiences resulting from amicable relations with others had reduced HB symptoms. Participants also stated that social support from others has helped them to deal with HB. Moreover, emotional stability and joy eased the emotional pain caused by HB, allowing them time to forget about HB.
“It was so much better when I went on a trip with my friends once in a while. Then, I got to calm down and forget things that made me suffer...”
(3) Exercise
Most participants responded that exercise helped them to recover from HB, as it reduced negative emotions and physical symptoms. The amount of exercise leading to decreased physical symptoms (i.e., negative emotions, hot flashes, and chest pressure) averaged at an hour of light intensity per day, such as walking. One patient in particular responded that HB improved greatly as her range and amount of movement increased after having knee surgery.
“I stroll around on this little hill in my town for an hour every day. This makes me breathe easier and feel refreshed.”
(4) Treatment
Most of the participants actively sought medical assistance for the physical symptoms of HB. Four patients’ symptoms were alleviated with Korean medicine, while two patients received medication from conventional psychiatrists. Two patients who believed that emotional problems were the cause of HB did not seek any treatment for HB their symptoms. Patients responded that they actively tried to alleviate their symptoms through appropriate treatment when those symptoms worsened.
(5) Inhibiting repetitive thinking via immersion
This factor refers to patients’ attempts to reduce and control repetitive thoughts and emotions by immersion in other activities. Some participants knew from experience that repetitive negative thinking aggravates HB and that reducing such thinking would alleviate HB their symptoms. Participants reported that external activities such as working or volunteering helped distract them.
“When I hung on to those things and kept on thinking about them, it became so hard for me...but HB became a lot better when I was taking care of the baby as I had something to care for and think about⋯so I volunteered back then.”
(6) Formation of positive self-image
Some participants responded that HB symptoms were alleviated as they started forming a positive self-image, often by finding their strength and having diverse experiences. This experience was formed mainly in social activities where people around them helped the participants to see themselves in a different way. This led the participants to form positive self-images, which ultimately helped them have a different perspective on life itself and react differently to stressors.
“People told me that I am good at working. I didn’t know that I had such talent, but I wanted to do better now, as people were starting to like me...It felt good to think that I’m actually a fine person. Then going to work got fun and it (HB) got a lot less painful.”
(7) Understanding other people
Some of the participants stated that they gained a higher level of human understanding by studying psychology and that they recovered from HB as they started understanding other people’s behavior. By understanding other people, participants were able to overcome becoming broken heart one-sidedly and accept differences between individuals. This led them to become hurt far less than before and obtain a semblance of emotional comfort. This understanding gradually helped them to recover from HB.
“I started to understand why these feelings emerged and how he must have felt. Learning how to understand and handle these things when I have certain feelings, I got much better.”
(8) Living for oneself
This factor denotes a change in lifestyle and values from dedication to others to living for themselves. Some participants responded that their condition became a lot better as the time they spent for themselves increased and they began following their own pursuits.
“I spend a lot of time for myself. it helped a lot spending time and money for myself.”
HB is a disease characterized by feelings of intense anger, often forged from continual stress relating to family matters or socio-economic problems, that leads to a series of physical and psychological symptoms such as chest pressure, hot flashes, surges of emotion and anger7). Women in a male-dominated society∓who are more likely to have fewer socioeconomic resources∓have a higher chance of suffering from this disease8). Conventional studies have also revealed that the majority of HB patients are middle-aged females3). HB commonly progresses in four stages, as follows: anger, conflict, resignation, and symptoms9). However, there is a dearth of studies involving the process of recovery, as well as the changes these patients go through.
Conventional studies have indicated that HB patients have a unique way of reacting to stress and their own psychological characteristics10,11). It is generally believed that HB patients utilize an inappropriate form of coping, which HB causes them to suffer from this disease as emotional stress persists. These patients are characterized by a unique reaction style of passive withdrawal and self-reproach12).
By maintaining an insight into the current condition of their disease9), many HB patients report that it was the prolonged suffering due to symptoms that caused them to realize that they had HB7). Participants in the present study also understood their current condition, but had a limited understanding of what would lead to their recovery.
In the majority of cases, recovery from HB was facilitated by external changes that triggered internal shifts in the patient’s mind. While some patients who were experiencing temporary stressors, such as monetary problems, demonstrated significant changes as the stressor was eliminated, others whose stressors could not easily be eliminated (e.g., those with family problems)were found to persistently suffer from HB.
Despite passively reacting to external stress during the development of the disease, HB patients often actively make various attempts to alleviate their symptoms. Conventional studies11) have reported that HB patients pursue problem-based support and religious measures. Participants in the present study also actively pursued solutions to the problem of HB by themselves through religion and vocation. When these attempts and adaptation strategies proved successful, patients experienced positive cognitive and emotional changes that, in turn, improved their manner of reacting to stress and their competence in dealing handling it. Thus, these changes resulted in the reduction of HB symptoms.
In addition, the social support received by patients appeared to relate their recovery from HB. Social support refers to types of information that make people believe that they are receiving love and respect from others and that they are invaluable members of a social relation network13). Patients could achieve adequate social support by revealing their thoughts about conflicts and stress to family, co-workers, friends, and religious groups. Reports have indicated that social support has a certain effect on self-respect14) and that it is negatively correlated with the symptoms and prognosis of depression15). Thus, it is possible to predict that social support plays a major role in recovery from HB.
Regarding emotional changes, it is thought that decreases in negative emotion, increases in positive emotion, and changes in how anger is expressed are related to HB recovery. These changes as a whole could be interpreted as emotional regulation. The fact that patients have difficulty in regulating their emotions means that they have difficulty recognizing and accepting their own emotions, lack regulatory strategies, and suffer behavioral problems from emotional pain16). Smooth emotional regulation can play both a regulatory and preventive role in depression17) and anxiety disorders18). It is thought that emotional regulation plays a major role in HB, as well, as patients also experience restrictions in everyday life due to emotional pain and failed emotional regulation.
Distinct emotional features of HB recovery include reduced anger due to decreases in impulsiveness, but also increases in the expression of anger. While some participants experienced a decrease in impulsive anger and actions through emotional regulation and the formation of counter-strategies, others tended to change their manner of anger expression as they experienced failure with a conventional strategy of holding back anger.
As a whole, the development of positive emotions and changes in cognition brought about changes in the environment and improvements in human relations, as internal changes affect activities and relationship with others. The severity of HB gradually lessens as those changes affect the internal development of patients via interactions with others.
However, patients in this study tended not to recognize that their HB symptoms were declining, and even thought that their symptoms had aggravated, viewing ordinary stress reactions as recurrences of HB. Perceiving ordinary reactions from stress in relation to HB, those patients formed a negative self-concept that they were susceptible or even hypersensitive to stress. This then made patients attribute a certain causative stress to an event, and even drove them to think that recovering from HB would not be possible without external changes. This process also made it difficult for patients to recognize the fact that their condition was actually improving. Moreover, it brought about despair, and even an increase in suffering, as patients started to believe that HB is a chronic disease that repeatedly recurs.
The significance of this study lies in the fact that the progress of HB patients was observed and that the process of change in female patients, who are thought to be weak in relative terms, was studied in depth through a series of interviews. In particular, the fact that HB patients did not perceive their declining symptoms as recovery of HB unless the causative stressor was removed helped provide a deeper psychological understanding of female HB patients.
Moreover, as there are a limited number of studies conducted on the recovery and prognosis of HB, the present study can provide impetus for future research involving the recovery process by offering insight into the factors relating to recovery as revealed by the inner experiences of HB patients in this study. The study is also expected to be helpful in providing a life index for HB patients.
However, this study lacks an objective index of the aggravation and changes of symptoms, as all symptoms in this study were reported qualitatively. In addition, one limitation of this study was the difficulty in recording the detailed changes in patients at the point of recovery, as the records were documented once a year during annual visits.
Further studies about the recovery period and prognosis of HB are expected to be carried out based on this study. It would also be possible to compile a life index and guidelines utilizing the factors and process of HB recovery.