A previous study showed that bee venom (BV) could cause anaphylaxis or other hypersensitivity reactions. Although hypersensitivity reactions due to sweet bee venom (SBV) have been reported, SBV has been reported to be associated with significantly reduced sensitization compared to BV. Although no systemic immediate hypersensitive response accompanied by abnormal vital signs has been reported with respect to SBV, we report a systemic immediate hypersensitive response that we experienced while trying to use SBV clinically.
The patient had undergone BV treatment several times at other Oriental medicine clinics and had experienced no adverse reactions. She came to acupuncture & moxibustion department at Semyung university hospital of Oriental medicine (Je-cheon, Korea) complaining of facial hypoesthesia and was treated using SBV injections, her first SBV treatment. SBV, 0.05 cc, was injected at each of 8 acupoints, for a total of 0.40 cc: Jichang (ST4), Daeyeong (ST5), Hyeopgeo (ST6), Hagwan (ST7), Yepung (TE17), Imun (TE21), Cheonghoe (GB2), and Gwallyeo (SI18).
The patient showed systemic immediate hypersensitive reactions. The main symptoms were abdominal pain, nausea and perspiration, but common symptoms associated with hypersensitivity, such as edema, were mild. Abdominal pain was the most long-lasting symptom and was accompanied by nausea. Her body temperature decreased due to sweating. Her diastolic blood pressure could not be measured on three occasions. She remained alert, though the symptoms persisted. The following treatments were conducted in sequence; intramuscular epinephrine, 1 mg/mL, injection, intramuscular dexamethasone, 5 mg/mL, injection, intramuscular buscopan, 20 mg/mL, injection, oxygen (O2) inhalation therapy, 1 L/minutes, via a nasal prong, and intravascular injection of normal saline, 1 L. After 12 hours of treatment, the symptoms had completely disappeared.
This case shows that the use of SBV does not completely eliminate the possibility of hypersensitivity and that patients who received BV treatment before may also be sensitized to SBV. Thus, a skin test should be given prior to using SBV.
Bee venom pharmacopuncture (BVP) refers to a type of treatment combining the efficacy of acupuncture with the biochemical pharmacological actions of bee venom (BV). The venom from live honey bees (
Hypersensitive reactions can be classified into four categories: local acute, local delayed, systemic acute and systemic delayed responses [4]. A systemic acute response is a kind of anaphylaxis. Anaphylaxis means that the symptoms suddenly appear when immune cells that have been sensitized to a specific antigen due to prior contact come into contact with the same antigen. The immunological response is that mast cells are activated by a specific antigen [5, 6]. A systemic acute response should be treated carefully because it may be accompanied dyspnea, airway obstruction, hypotension, syncope and dizziness [7, 8], which may result in an emergency.
Sweet bee venom (SBV) is intended to address the above issues. SBV is BV with antigens, such as certain enzymes and histamine, removed [9]. In previous studies, SBV has been shown to have a reduced risk of anaphylaxis and allergic reactions [10, 11]. Although studies on anaphylaxis have mostly been related to BV [12, 13], local reactions with normal vital signs [14] and combination BV therapy [15] have been reported with respect to SBV anaphylaxis. However, no systemic immediate hypersensitive response accompanied by abnormal vital signs has been reported with respect to SBV. We report a case in which a systemic immediate hypersensitive response occurred while trying to use SBV clinically. The details contained in this report should contribute to the safer use of SBV.
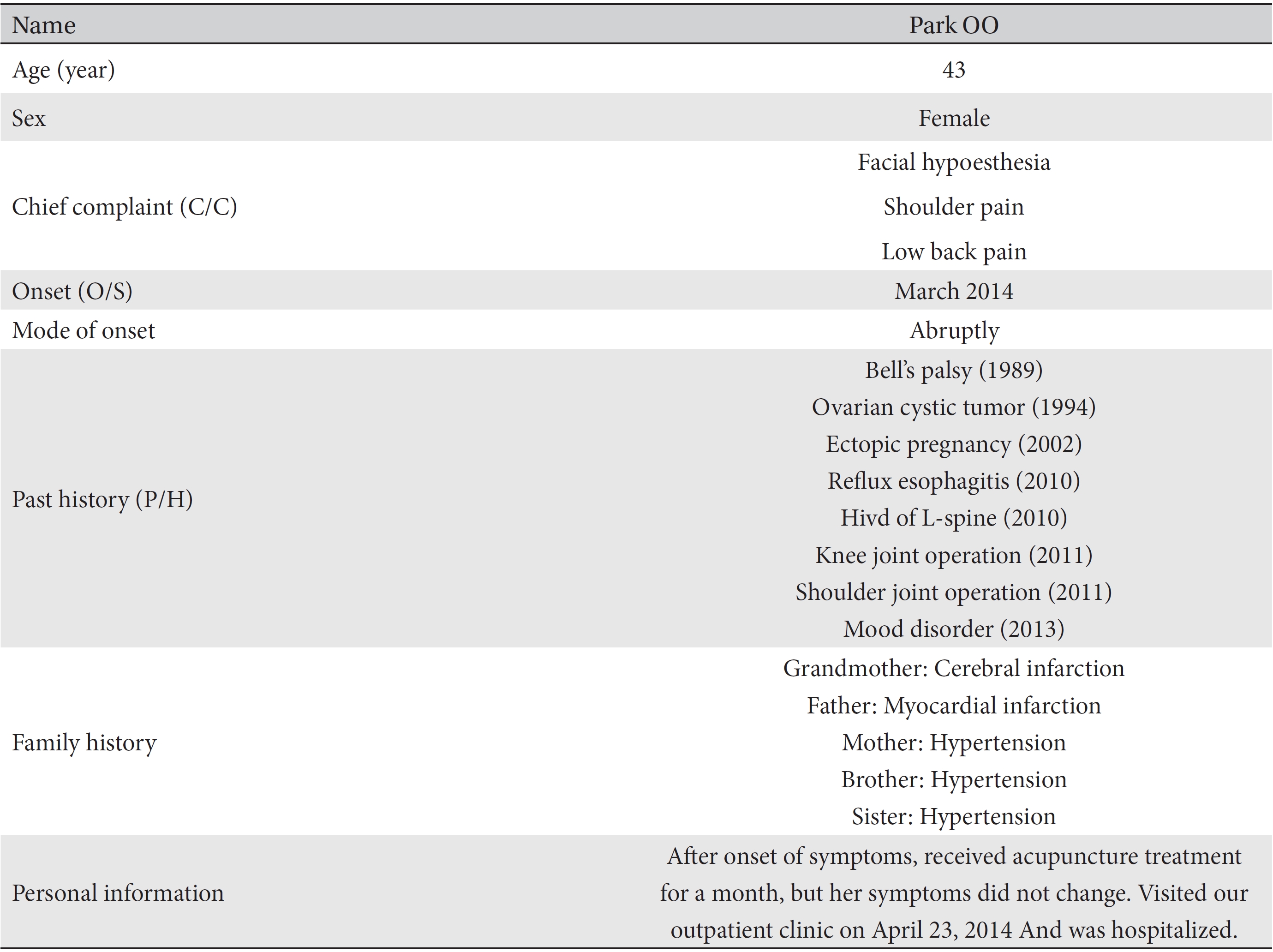
The patient, a 43-year-old female, visited out hospital on April 23, 2014. The patient’s medical history and other pertinent information were obtained (Table 1), and after an examination, the patient was admitted to acupuncture & moxibustion department at Semyung university hospital of Oriental medicine (Je-cheon, Korea). Three days later, on April 26, the symptoms of facial hypoesthesia were still the same. In the morning two days later, April 28, a decision was made to use SBV. That afternoon (1:25 pm) SBV treatment was started, with 0.05 cc of SBV being injected at each of the following 8 acupoints, for a total dose of 0.40 cc: Jichang (ST4), Daeyeong (ST5), Hyeopgeo (ST6), Hagwan (ST7), Yepung (TE17), Imun (TE21), Cheonghoe (GB2), and Gwallyeo (SI18). Almost immediately after the SBV treatment (2:25 pm), the patient complained of hot flashes in her palms and face. She also complained of itchy palms and soles. No other complaints, such as edema, dyspnea, or sweating, were noted. An ice pack was applied.
She was going to be sent to a ward for her condition to stabilize, but suddenly she sat down and complained of abdominal pain. Her vital signs were as follows: a blood pressure of 100/60, a pulse rate of 84 beats per minute, a respiration rate of 20 breaths per minute, and a temperature of 36.5°C (100/60, 84, 20, 36.5). She complained of nausea with lower abdominal pain and a squeezing feeling. She could not stand up because of dizziness and general body weakness, she was perspiring profusely, and her complexion was pale. She was taken to the emergency room on a stretcher (2:30 pm).
In the emergency room, epinephrine, 1 mg/mL, was injected intramuscularly. The patient remained mentally alert, but her vital signs had changed (40/-, 58, 22, 36.5). The patient was unable to straighten her legs while lying on her side because of abdominal pain. She continued to complain of nausea, chest discomfort and dyspnea. Dexamethasone, 5 mg/mL, was injected intramuscularly. The patient remained mentally alert, with vital signs of 40/-, 54, 24, 36.3 and oxygen saturation (SPO2) of 98%. The patient still complained of abdominal pain, nausea, chest discomfort and dyspnea, and she was perspiring profusely over her entire body. Buscopan, 20 mg/mL, was injected intramuscularly, and oxygen (O2) inhalation therapy at 1 L/minutes via a nasal prong was administered (2:45 pm). Her blood pressure improved to 80/60, her other vital signs were 52, 24, 36.2, and her SPO2 remained at 98%. She still complained of abdominal pain and coldness in her body, but her rate of perspiration was reduced.
Slightly later (3:00 pm), although she continued to complain of abdominal pain, nausea, and coldness, her rate of perspiration was reduced, and her chest discomfort and dyspnea had disappeared. At that time, her vital signs were 130/80, 110, 24, 35.8. Because the patient continued to complain of severe abdominal pain, nausea, and coldness, a hot bad was applied (3:15 pm), followed 15 minutes later by infrared treatment (3:30 pm). About one-half hour later (4:00 pm), she continued to complain of abdominal pain, coldness and nausea, but the abdominal pain was slightly relieved. The patient then complained of palpitations, so an electrocardiography (EKG) was done and showed sinus arrhythmia, varied rate 49 ─ 76, borderline st elevation, and inferior leads. After another one-half hour (4:30 pm), the abdominal pain was reduced, the nasal prong was removed, and the supine position was possible; however, she still complained of coldness, so the infrared treatment was continued. Thirty minutes later (5:00 pm), her SPO2 dropped, so the nasal prong was re-inserted and O2 inhalation at 1.5 L/minutes was started for the second time. However, the patient continued to complain of whole body weakness, so 1-L of normal saline was administered via intravascular injection (5:10 pm). By 6:00 pm, the abdominal pain, nausea and coldness were relieved so the infrared treatment was stopped. However, because the patient still complained of entire body weakness, the normal saline intra- vascular injection was continued. By 6:30 pm, the patient experienced only a stabbing pain around her navel, and she was capable of autonomous postural changes. At 7:00 pm, only a slight abdominal pain remained, and the nasal prong was removed. At that time, her vital signs were 100/60, 68, 20, 36.5.
Over the next several hours, her symptoms continued to reduce in severity. By 7:30 pm, her nausea had disappeared, and at 8:30 pm, she autonomously changed positions in bed. By 9:30 pm, her chest discomfort had disappeared, at which time her vital signs were 100/60, 80, 20, 36.6. At 1:30 am, although a little abdominal pain remained, the patients tried to sleep. At 2:00 am, the patient was asleep, and her respiration was stable. Her vital signs at that time were 100/70, 78, 20, 36.6.
Anaphylaxis is an extreme systemic hypersensitivity reaction. Immediate hypersensitivity reactions occur very rapidly, and vessels and smooth muscles involving the immunoglobulin E (IgE) antibody and mast cells are concerned. Inflammation, such as swelling and hot flashes, is often present. Such a reaction occurs in people previously exposed to an antigen, and a second exposure to that antigen can lead to a wide range of mast-cell activities. Fluid leaves the blood vessels, causing a swelling of tissues and a decrease in the blood pressure, possibly leading to shock. Death from anaphylaxis is caused by airway constriction or epiglottis edema. In the United States, more than 160 people die from it every year. Insects, such as wasps, bees, or other poisonous insects, account for 25% of the cases of anaphylaxis [16,
In a previous study, BV was reported to cause anaphylaxis [8, 12] and other hypersensitivity reactions [4]. The major allergenic components of BV are phospholipase A2 (PLA2) and histamines. The active ingredient of BV with the allergic components removed is the nucleus of SBV, with more than 10,000 components being removed from BV during the manufacturing process of SBV. Because melittin is the most important active ingredient of BV, SBV is made to isolate melittin to minimize patient discomfort [9,
The patient in this case had been treated with BV at other Oriental medicine clinics. At those times, she had no adverse reactions to BV. After coming to our clinic, she received her first SBV treatment of 0.05 cc of SBV injected at eight different acupoints for a total dosage of 0.40 cc. Hypersensitivity reactions occurred abruptly about one hour after the treatment. The main symptoms were abdominal pain, nausea and perspiration, but symptoms commonly associated with hypersensitivity, such as edema, were mild. The patient while lying on her side and bent at the waist was unable to straighten her legs because of stomach pain. Abdominal pain accompanied by nausea was the most long-lasting symptom. Her body temperature went down due to profuse sweating, and her diastolic blood pressure could not be measured on three occasions. No feces or urine incontinence was noted, and she was mentally alert during the entire time that the symptoms per sisted.
In previous studies on the side effects of SBV, itching or hot flashes were reported, but no abnormal vital signs, such as abnormalities in blood pressure, body temperature, respiration rate or pulse, were noted. In previous studies on the side effects of BV, swelling, perspiration, a body barrel, itching or hot flashes were reported. However, to date, no cases of systemic immediate hypersensitive reactions to SBV, for which the main symptom is abdominal pain, have been reported [12, 13].
The main symptoms of anaphylaxis are swelling, skin redness, wheal response, perspiration, itching and dyspnea. The abdominal pain is mainly caused by an antigen from food penetrating the digestive system [
Although this report involves only a single patient, it is different from previous ones because systemic reactions, abnormal vital signs and abdominal pain have been identified as possible side effects of treatment with SBV. This case clearly demonstrates that hypersensitivity reactions cannot be completely prevented by using SBV and that patients who have received BV treatment before may be sensitized to SBV. Thus, a skin test should be administered prior to using BV.
[Table. 1] Patients basic information
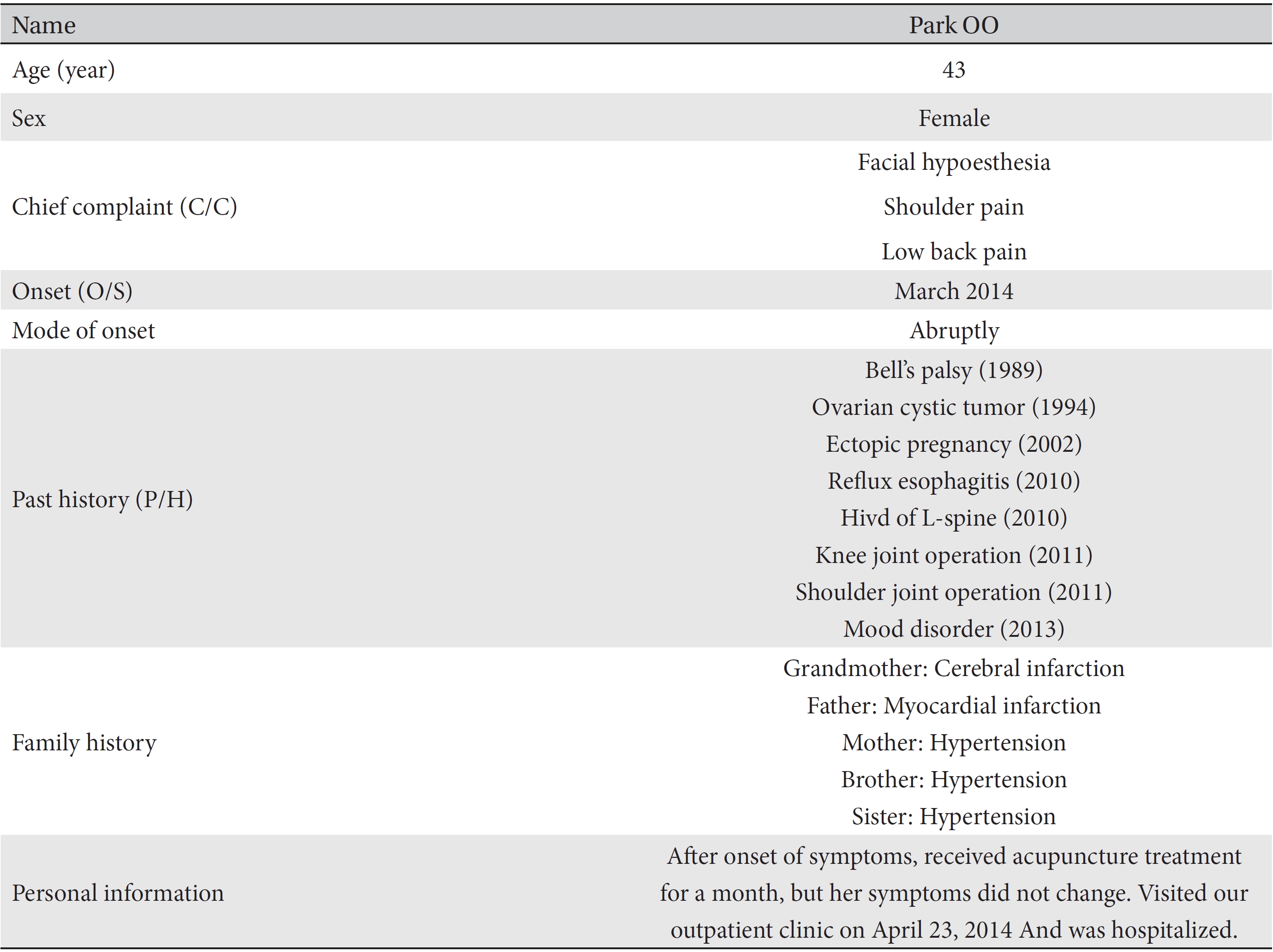
Patients basic information