The present study evaluated the effects of sa-am acupuncture (SAA) simpo-jeongkyeok (SPJK) treatment on the blood pressure (BP), pulse rate (PR), and body temperature (BT) of patients with hwa byung (HB).
This patient assessor blind, randomized, placebo controlled trial included 50 volunteers, divided randomly into two groups. The treatment group underwent SPJK (PC9, LR1, PC3, KI10) while the control (sham) group received minimal needle insertion at non acupoints. The BP in both arms, PR, and BT at several acupoints were measured before and after treatment at the 1st, 2nd, 3rd, and 4th visits and before treatment at the follow-up visit. We analyzed data by using the repeated measured analysis of variance (RM ANOVA), Mann-Whitney U, and wilcoxon signed rank tests; differences at P < 0.05 were considered significant.
No significant differences in the systolic blood pressure (SBP), diastolic blood pressure (DBP) and PR between the treatment and control group were observed at each visit. However, the decrease in the SBP for the treatment group before and after each visit was significantly higher than it was in the control group. The SBP in both arms in the treatment group was decreased between visits 1 and 2, 1 and 3, 1 and 4, and 1 and follow-up. The DBP in both arms and in the right arm between visits 1 and 3 in the treatment group showed decreases. A minimal BT increase for treatment at CV06 and CV12 and a minimal BT decrease for treatment at CV17 and (Ex) Yintang were found. Patients in the treatment group who visited more frequently experienced a greater decrease in the PR, but that effect was not maintained.
The results suggest that SAA SPJK treatment has instant positive effects on the BP, PR, and BT in patients with HB, but the effects on the BP and PR are not maintained.
Hwa byung (HB, 火病) is a disease caused by continuous stress and the inhibition of bad emotions such as depression, anger, and so on. HB produces various psychological and somatic symptoms, including depressed mood, anxiety, pushing up in the chest, chest tightness, fatigue, headaches, dizziness, mouth dryness, insomnia, palpitation, indigestion, and so on. HB literally means “anger disorder” or “fire disease” because ‘Hwa’ means anger or fire and ‘byung’ means disease or disorder. HB is a Korean culture related syndrome related to a deep expression of feeling, i.e., deep sorrow (恨), and is included in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) [1, 2]. Sa-am acupuncture (SAA) is a unique Korean acupuncture method that was developed by a Korean hermit, master sa-am, in the sixteenth or seventeenth century A.D. and is now one of the popular acupuncture techniques used in Korean traditional medicine [3, 4].
The pericardium is known to control blood circulation in the entire body indirectly and to assist and protect the heart by defending it against the invasion of pathogens (邪 氣). The pericardium is involved in the action of the mind and regulates emotion. In SAA methods, the pericardium meridian, which is connected to the pericardium, is used to treat heart diseases, circulation disorders, and neuropsychiatry diseases [5, 6]. Simpo-jeongkyeok (SPJK, 心包正格) is a SAA method that tonifies LR1 and PC9, and sedates KI10 and PC3, and that is used to tonify a deficient pericardium meridian and a deficient function of the pericardium [3, 4]. SPJK treats the deficiency syndromes of mental disease, such as non stopping of joy and laughter, delirious speech, anxiety, nervousness, and so on [7]. Several randomized controlled trials (RCTs) have been conducted to prove the effects of SAA a for treating hypertension [8], chronic tension type headaches [9], dysmenorrhea [10], simple obesity [11], and HB [12-14].
We already reported that SPJK, from among SAA methods, was effective for treating HB [14]. However, we also theorize that SAA may have an effect on the blood pressure (BP), pulse rate (PR), and body temperature (BT) because SAA has been shown to have positive effects when is used to treat HB, as well as hypertension. Thus, the purpose of the present study was to examine additionally in a RCT the effects of SAA SPJK treatment on the BP, PR and BT in patients with HB [14].
The study was a patient assessor blind, randomized, placebo, controlled trial and included 50 women aged 20 ─ 65 years who visited Sangji Korean Medicine Hospital from May 2010 to October 2010 and were diagnosed as having HB by using the Hwa Byung Diagnostic Interview Schedule (HBDIS). This study was conducted according to the ethical standards of the Helsinki Declaration. After the study protocol had been approved by Institutional Review Board of Sang-Ji University Korean Medicine Hospital (No. SJ IRB 100512), informed consents were obtained from the subjects. Patients with HB for less than a 6 month duration, with a psychosis such as delusion, hallucination and mania, or with a history of alcohol and drug abuse were excluded. Because disorders such as liver, heart, endocrine, and kidney disorders may occur with HB, patients who had those disorders or who were taking medications for those disorders were also excluded. Pregnant women and lactating women were determined not to be appropriate for this study. Patients who drank alcohol or beverages containing caffeine, who overworked the day before the experiment, or who had undergone acupuncture treatment or had participated in other clinical experiments during the previous one month were excluded. Patients who had knowledge of acupoints and acupuncture effects were excluded as well. Others who were thought to have difficulties in performing the experiment were excluded.
The number of women in one group was arbitrarily decided as 20 women without analyzing the sample size because the study was a pilot study. The target sample sizes for the treatment and the control groups were 25 women each, considering a dropout rate (20%). The subjects were randomly assigned by using statistical analysis system (SAS) program (ver. 9.1.3) into those who would receive real acupuncture (treatment group) and those who would receive minimal sham acupuncture treatment (sham or control group) in a 1 : 1 ratio. The subjects were numbered and listed at random. The random code list was sealed in a double non penetrable envelope, and the envelope was opened just before the experiment. The volunteers, data collector and analyst were unaware of the individuals who would be receiving the treatment. The procedure in both the treatment and the control groups was done by one Korean doctor for consistency. Only one analyst, who did not know the assignment of subjects, analyzed the data taken before and after treatment.
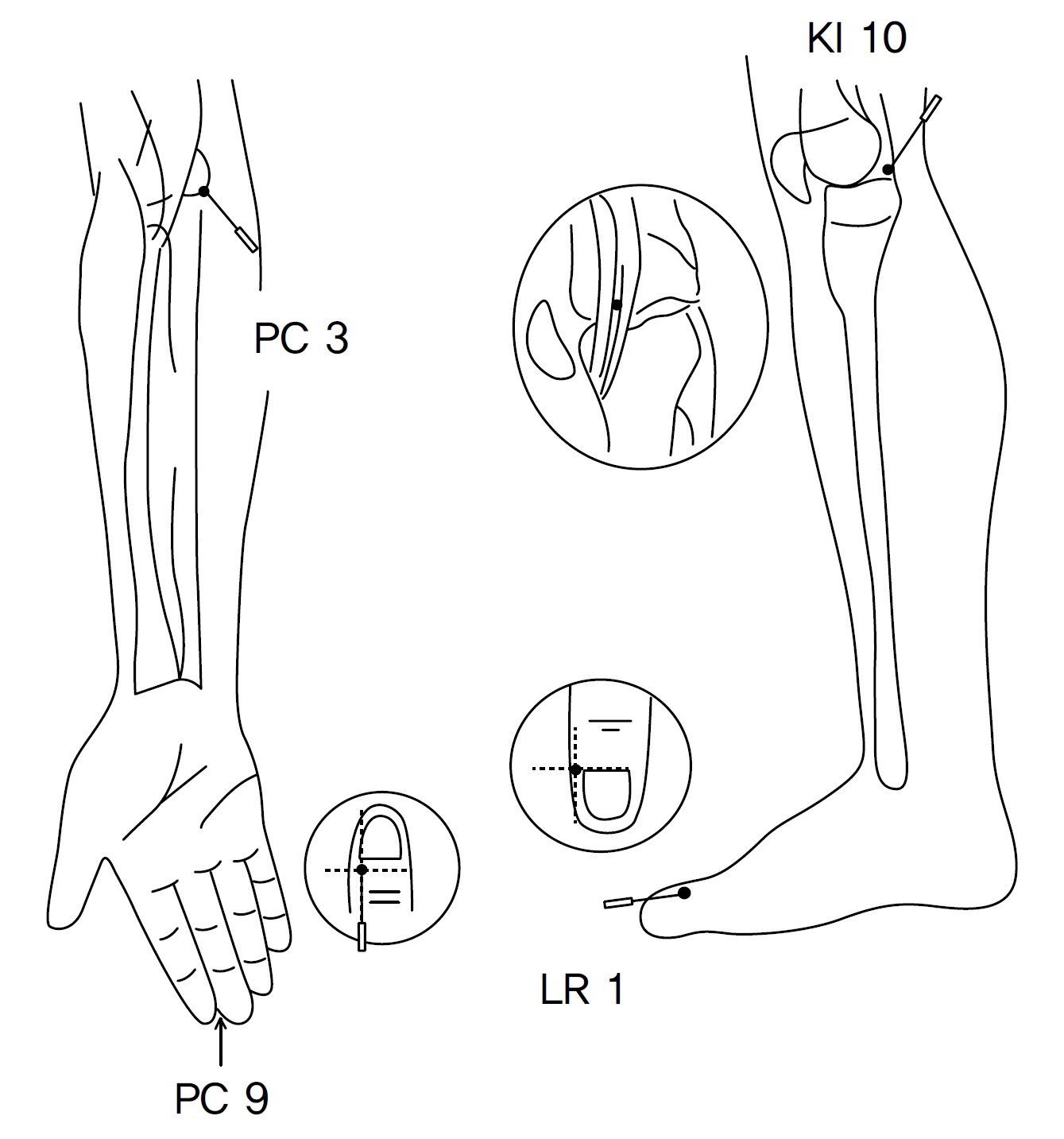
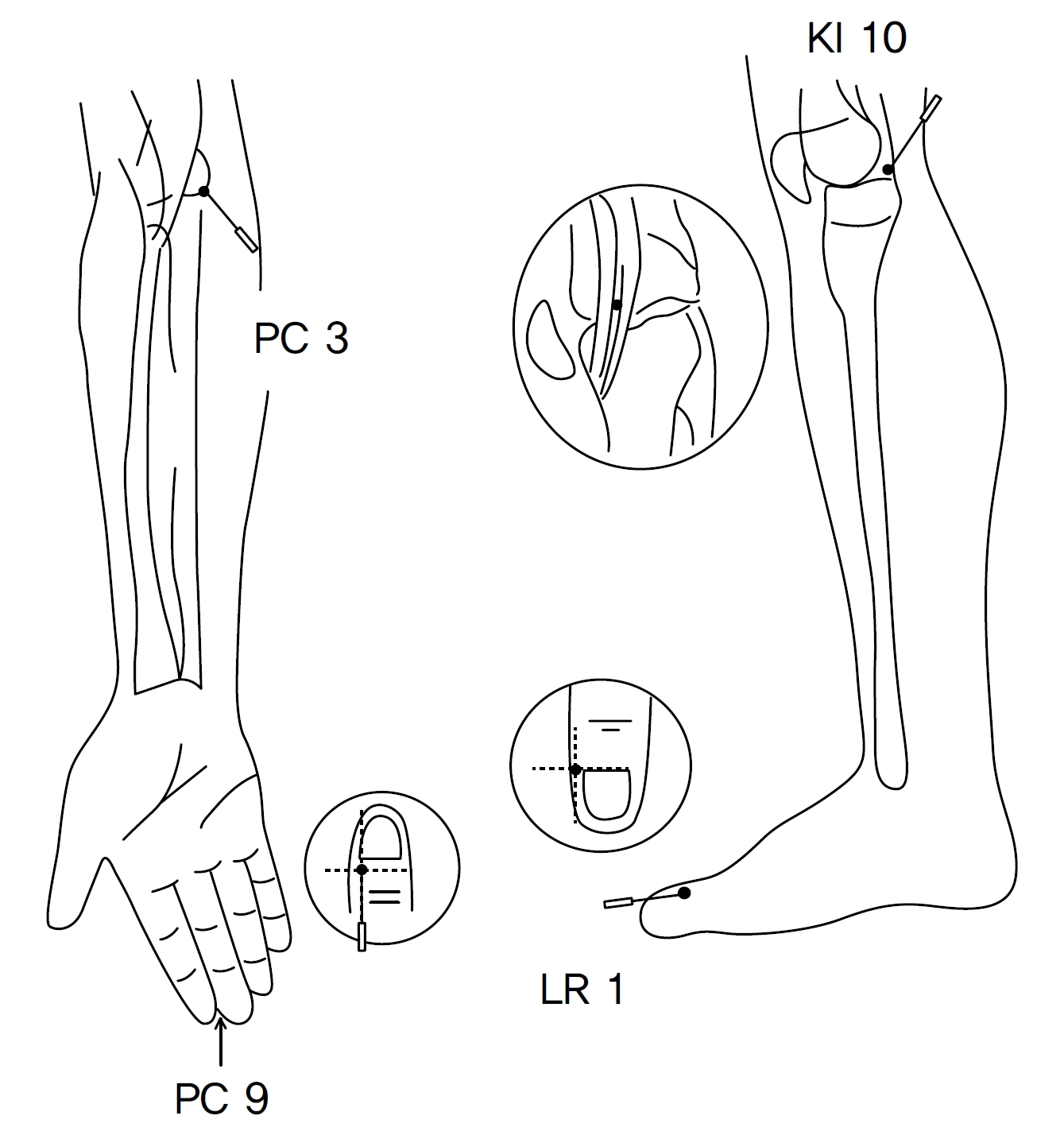
For the treatment group, sterilized, single use needles (0.25 mm × 30 mm, stainless steel, Dongbang, Korea) were used for the intervention. Totally, four treatments over 2 weeks were done at the same time of the day. Acupuncture was done for 20 minutes. No other treatments were done. The treatment group underwent SAA SPJK treatment (Fig. 1) Needle insertion was done at PC9, LR1, PC3, and KI10 on the right side. Insertions of 2 ─ 3 mm at PC9 and LR1 and of 10 mm at PC3 and KI10 were used. Directional supplementation and draining (DSD, 迎隨補瀉) and de- Qi were performed (Fig. 1) The control group underwent sham acupuncture at non acupoints. Needle insertions with depths of less than 3 mm depth were done at 6 cm superior and 3 cm lateral of PC3, 6 cm superior and 3 cm medial of PC3, 6 cm inferior and 3 cm posterior of KI10, and 6 cm inferior and 3 cm posterior of GB34. DSD and de-Qi were not performed.
Demographic information such as the medical history, age, height, weight, drinking and smoking habits, and medications being taken was checked at the first visit. The BP and the PR were measured before and after treatment at visits 1, 2, 3, and 4 and before treatment at the follow-up (f/u) visit (visit 5). BT at (Ex) Yintang, CV17, CV12, and CV6 were measured before and after treatment at visits 1 and 4 and before treatment at the f/u visit. The HEM-7200 unit (OMRON, Japan) was used to measure the BP and the PR. The BT was measured with a 01500 infrared thermometer (THERMOFOCUS, Italy). Data were recorded as means ± standard deviations (SDs). We analyzed the data by using the Mann-Whitney U, wilcoxon signed rank, and repeated measured analysis of variance (RM ANOVA) tests and considered statistical significance at
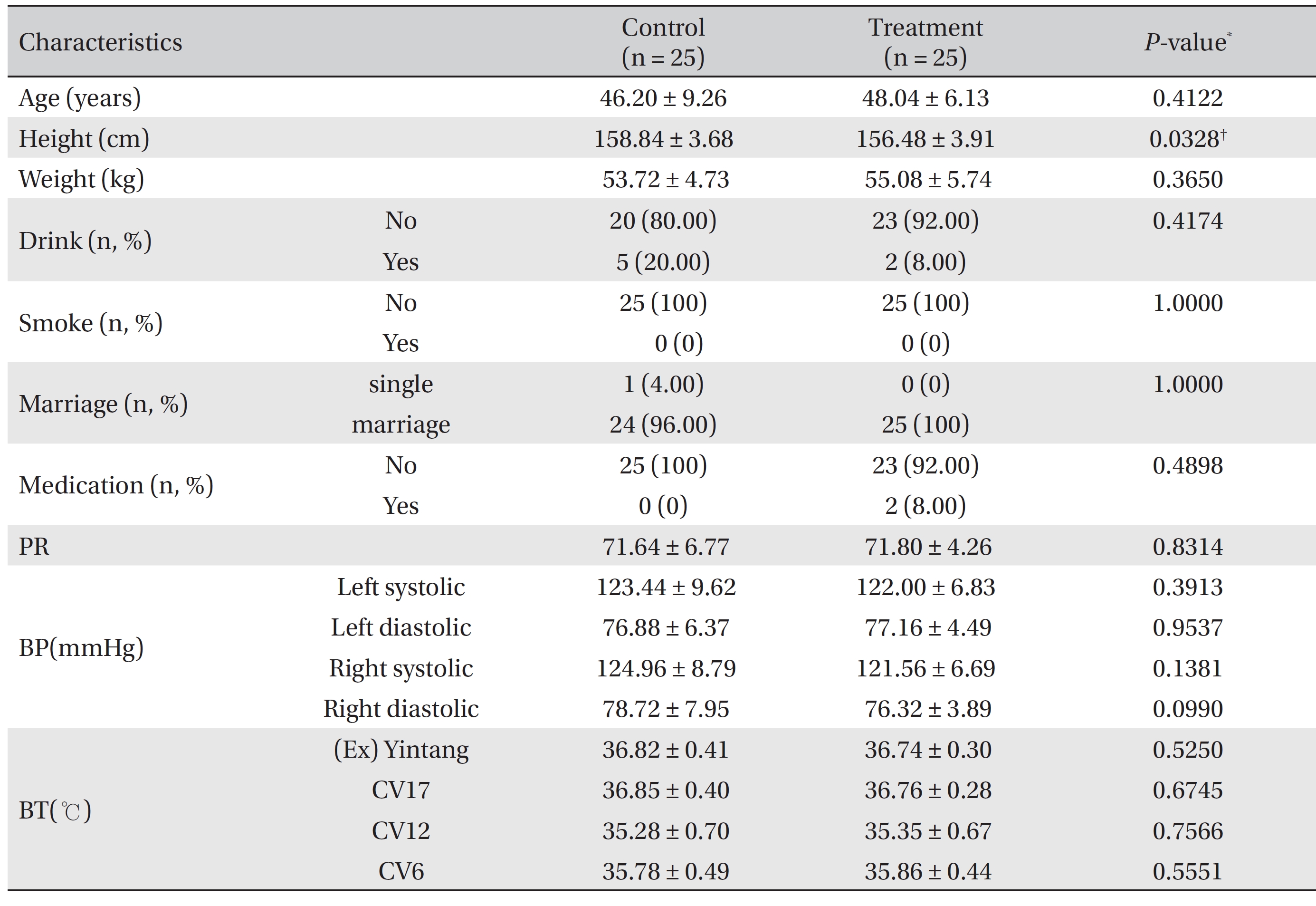
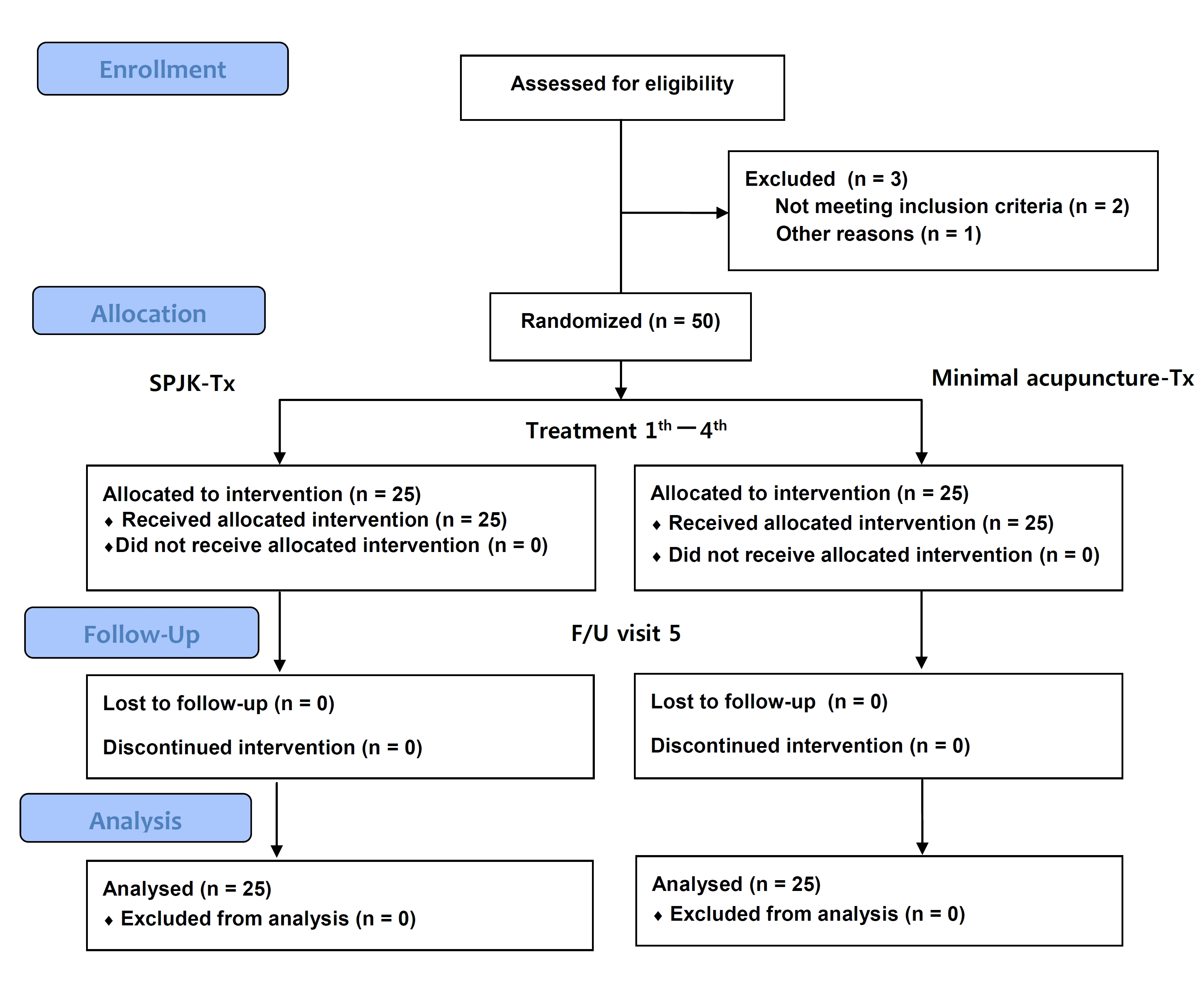
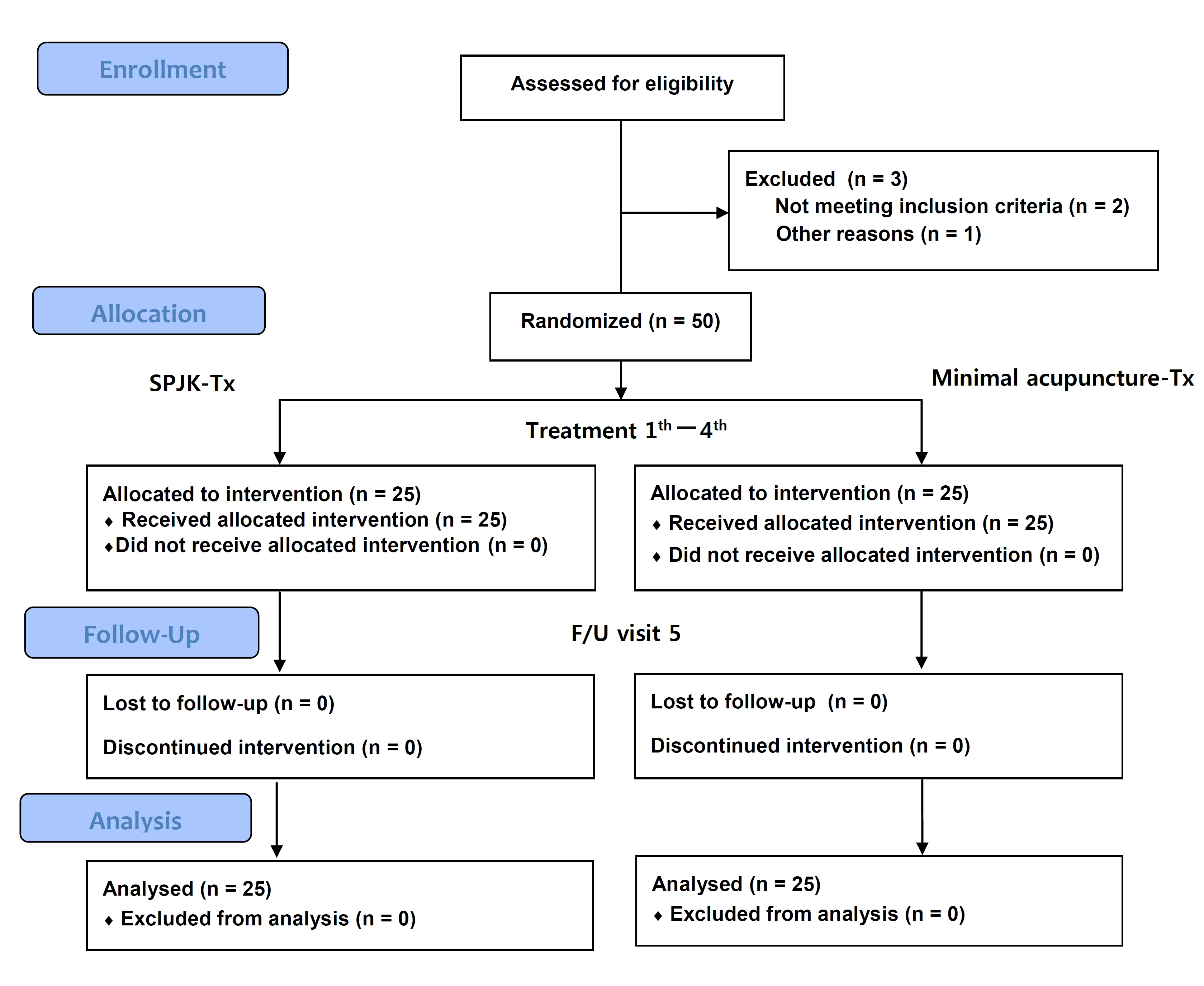
Two participants who did not meet the inclusion criteria and one participant with endocrine disorder from among the 53 participants at the screening step were excluded. Fifty participants were finally enrolled and finished the trials; there were no drop outs. Twenty five participants each were randomly place into the SPJK treatment group and the control group (Fig. 2) On the baseline characteristics, no significant differences in age, weight, drinking and smoking habits, marriage, medication, PR, both side systolic and diastolic BP, and BT were noted between the treatment and the control groups. The average height in the control group was 2.36 cm larger than that in the treatment group (156.48 ± 3.91
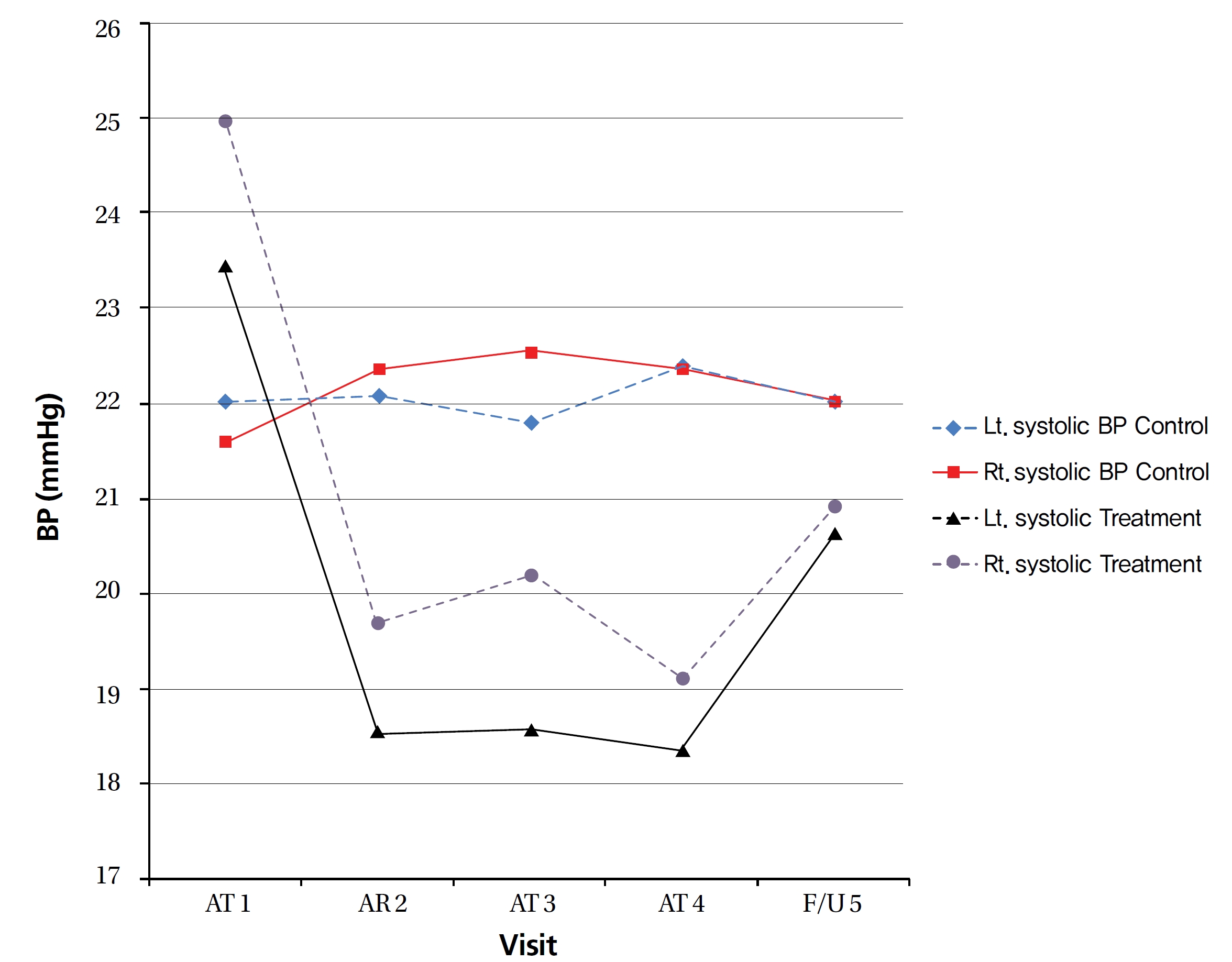
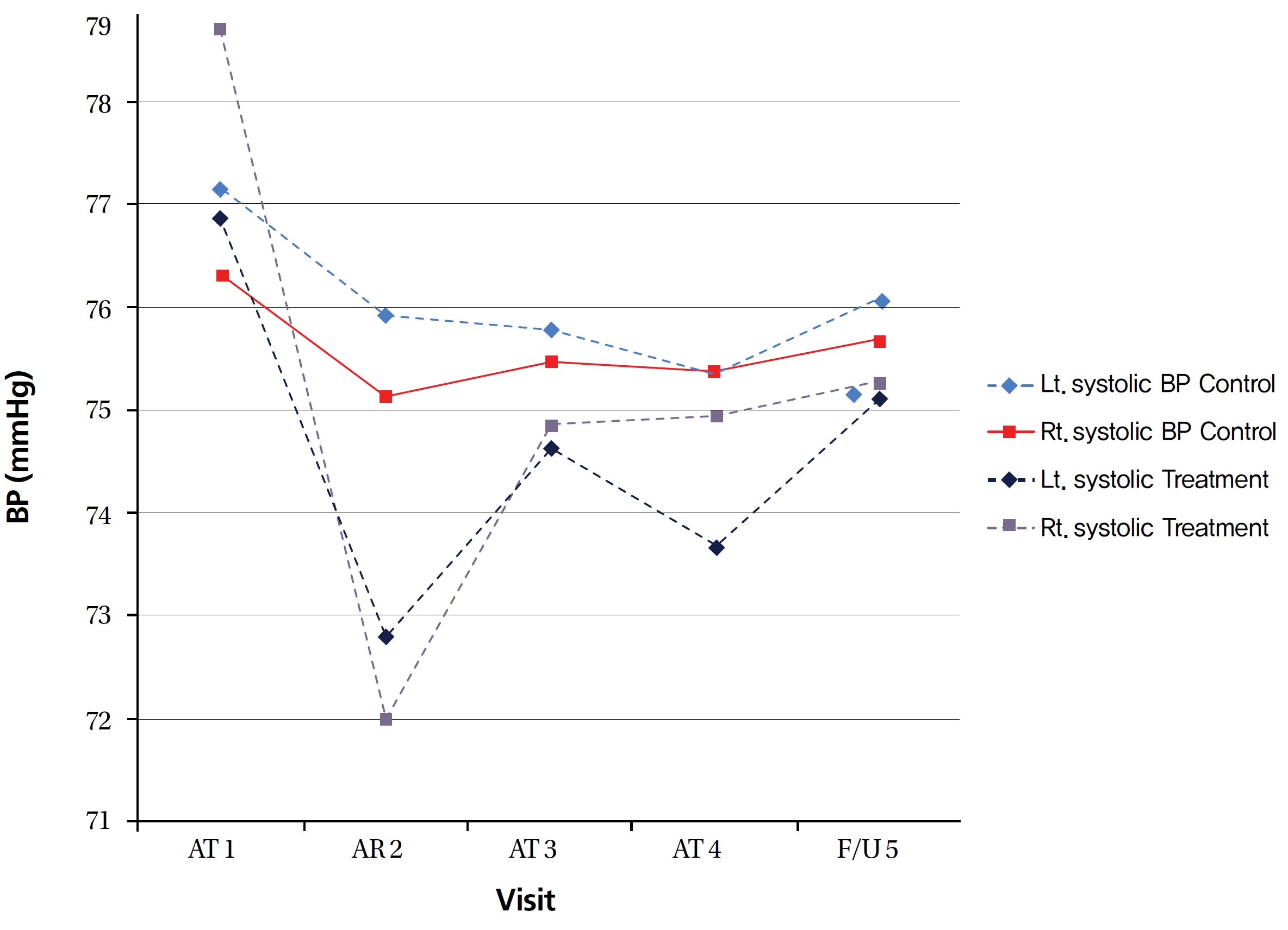
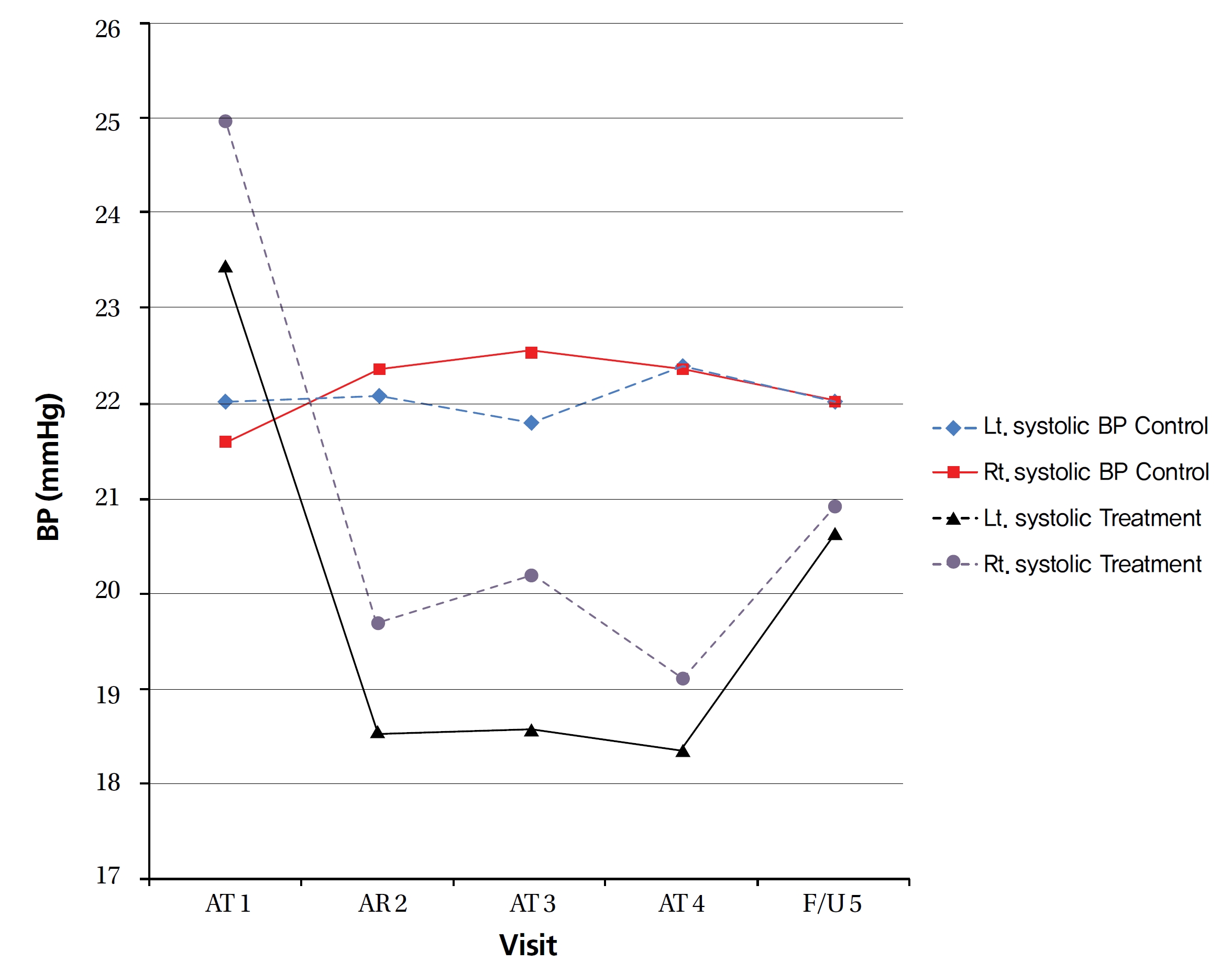
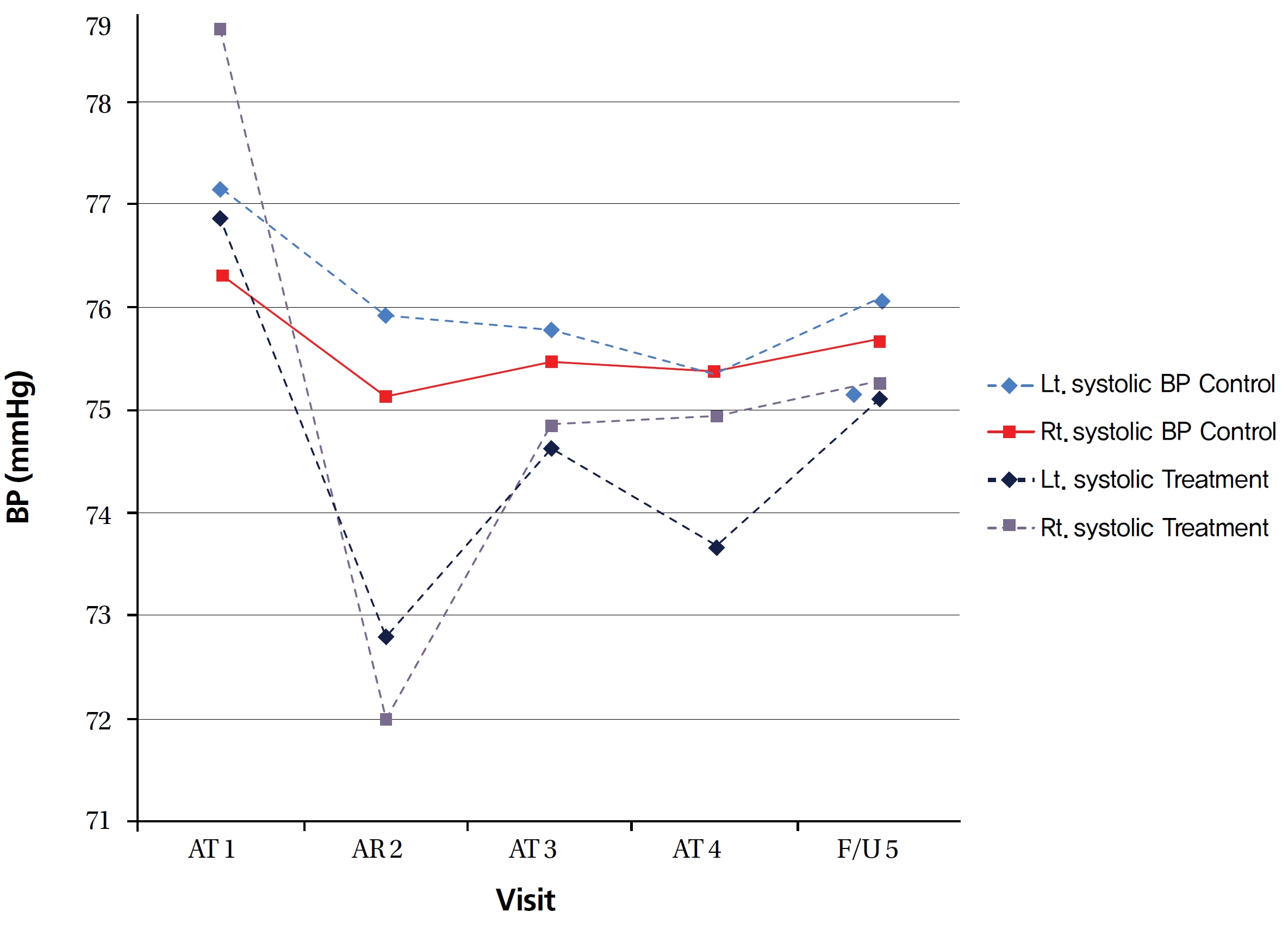
The right (Rt.) and the left (Lt.) side systolic blood pressure (SBP) of the treatment group showed 4.2% and 4% decreases, respectively. The decrease in the both side SBP continued until visit 4. Until the f/u visit, the decrease in the Lt. side SBP was minimal and the decrease in the Rt. side SBP was maintained. However, no significant differences in the SBP and the diastolic blood pressure (DBP) in between the control and the treatment groups were observed at each visit (RM ANOVA, SBP within group
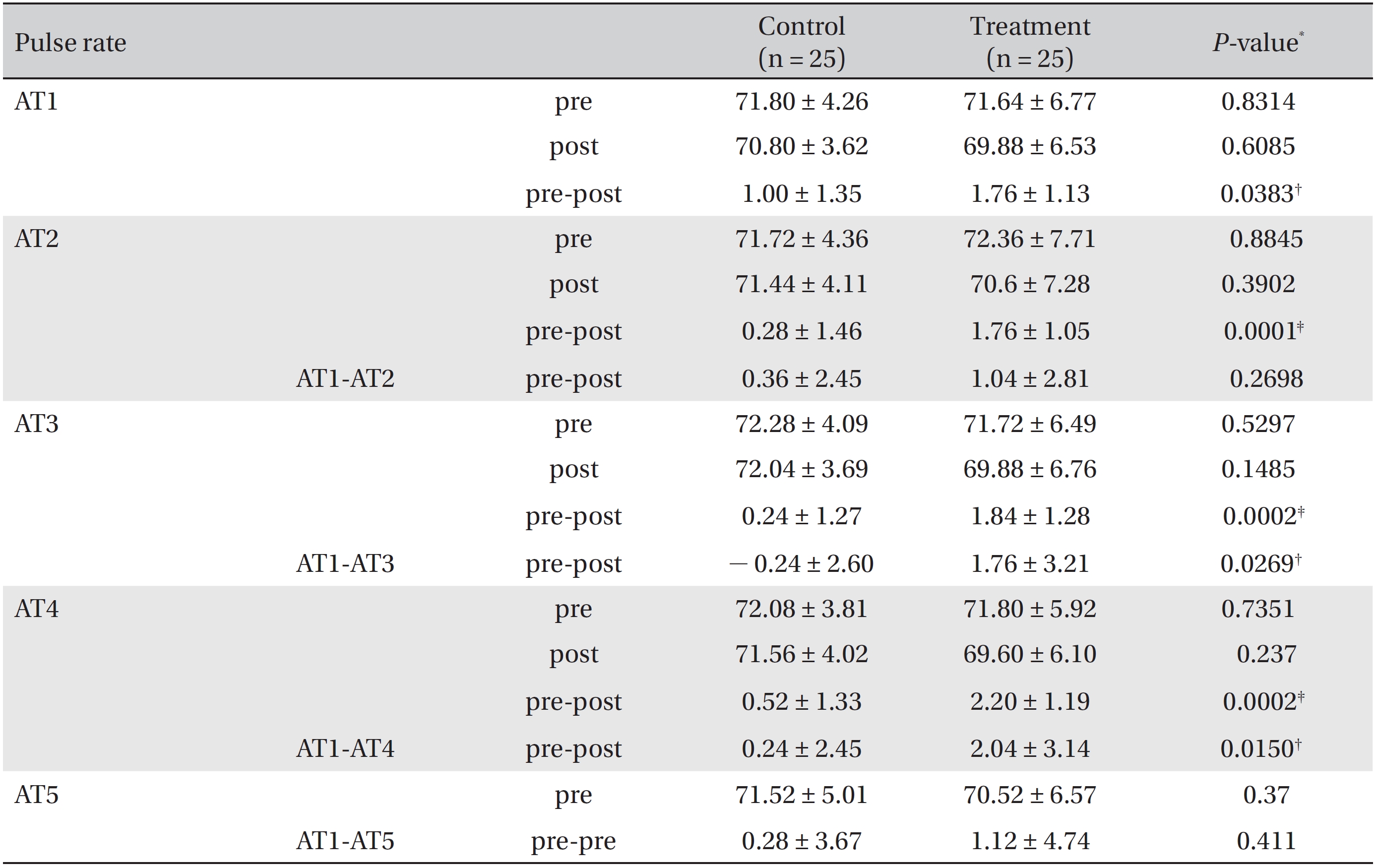
The differences in the PR between before and after treatment at each visit between the treatment and the control group were significant (Table 4), but that decrease in the PR did not continue until the f/u visit. The PRs of the treatment and the control groups showed no significant differences at each visit (RM ANOVA, within group
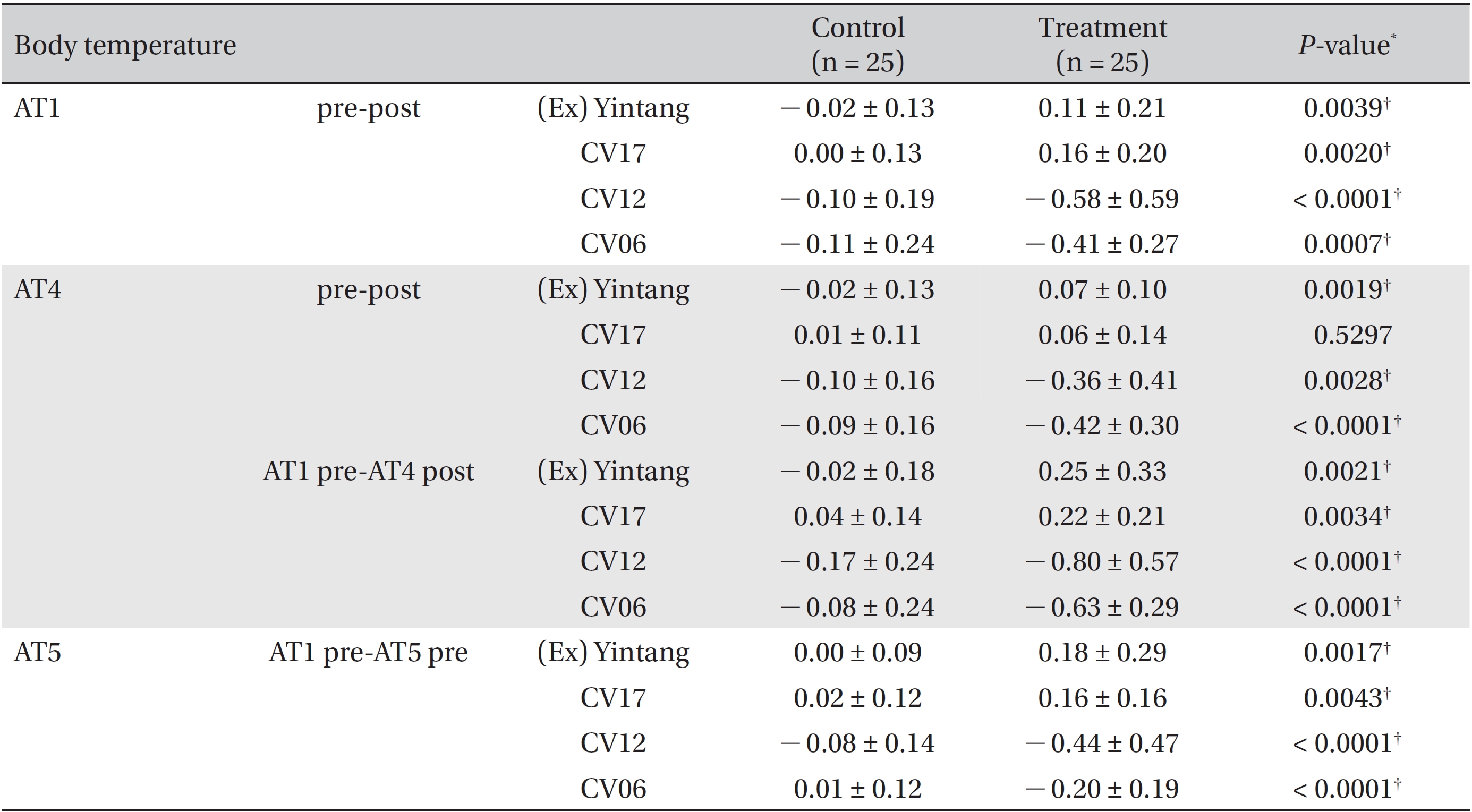
The BTs at (Ex) Yintang, CV17, CV12, and CV06 at each visit showed significant differences within groups (RM ANOVA,
Several RCTs studying the effects of acupuncture in lowering the BP have been reported [8, 15-18]. Some studies suggested that acupuncture might have reduced the BP in patients with hypertension [8, 15-17] whereas others reported contradictory results [18]. Thus, the effect of acupuncture in lowering the BP is still controversial. However, acupuncture has been reported to lower the BP significantly in patients taking antihypertensive medications [19]. Many studies have indicated that acupuncture might be a good adjunctive therapy for treating hypertension [19, 20].
Our study’s conditions were not similar to those of other studies [8, 15-20] because the patients in our study were patients with HB, but not with hypertension. This study showed that immediately after treatment acupuncture without an antihypertensive drug had decreased BP compared to the normal range of BPs, but that effect was not maintained. Our study’s results were similar to those of Chen
The acupuncture mechanisms for lowering the BP are unclear. However, electroacupuncture has been reported to activate neurons in the hypothalamic arcuate nucleus, the ventrolateral periaqueductal gray matter (vlPAG) in the midbrain, and the nucleus raphe in the medulla to inhibit the neural activity in the rostral ventrolateral medulla (rVLM) and to inhibit the reflex hypertension through opioid mediated inhibition of glutamate in the rVLM [22, 23]. Another report suggested that acupuncture might regulate the cardiovascular system through a complicated brain network from the brainstem, the hypothalamus, and the cortical level [21]. Some evidence suggests that acupuncture lowers the BP by modulating the activity of cardiovascular pre-sympathetic neurons in the rVLM [24] and can improve the circadian rhythm of the BP in patients with hypertension by normalizing the decreased parasympathetic nerve activity [15, 25, 26] or by regulating the autonomic nervous system (ANS) [27-29].
Sympathetic nerve stimulation (SNS) increases the heart rate (HR) and the PR, and constricts both the heart and all the blood vessels of the systemic circulatory system. SNS increases the resistance to venous return and the mean systemic filling pressure. Conversely, parasympathetic nerve stimulation (PNS) or the inhibition of SNS causes the opposite effects [30]. We speculate that the BP and the PR decrease because the hyperactivity of SNS caused by HB is inhibited or because PNS is activated by SAA SPJK. A report that the SAA method of supplementing LR1 and draining KI11 significantly decreased the mean artery pressure in normal rats [31] supports our study’s results.
The BT is regulated by nervous feedback mechanisms operating through temperature regulating centers in the ANS of the hypothalamus. PNS or the inhibition of SNS increases blood flow to abdominal organs such as the gastrointestinal tract and the kidneys [30]. We postulate that the abdominal temperature (CV12 and CV06) increases whereas the face and the chest temperatures ((Ex) Yintang and CV17) decrease because SPJK activates PNS, which induces an increase in the blood flow at abdominal organs.
Our study was limited by its being a small sample size clinical trial. A larger sample size is necessary because more concrete conclusions are to be drawn. Second, the acupuncture treatment and the follow-up duration were each two weeks. The duration of our study was shorter than that of clinical experience and a large clinical trial. Nevertheless, the present study demonstrated that SPJK could lower the BP, decrease the PR, and maintain homeostasis of the BT soon after treatment. Third, the subjects of this study were patients with HB and normal BP (not with hypertension). Thus, we were unable to ascertain whether the SPJK treatment had a real effect in lowering the BP or the lowering of the BP was an effect accompanying the treatment of HB. However, we were able to determine that SPJK had an immediate effect on the BP, PR, and BT in the normal range and that the effect could not be maintained, although a precise conclusion could not be drawn from this study. Future rigorous RCTs with larger sample sizes and long durations are recommended to identify the effect of SAA SPJK treatment in lowering the BP in patients with hypertension.
The results of this study suggest that SAA SPJK treatment has instant positive effects on the BP, PR, and BT in patients with HB, but the effects on the BP and PR are not maintained.
[Table. 1] Clinical characteristics of the subjects
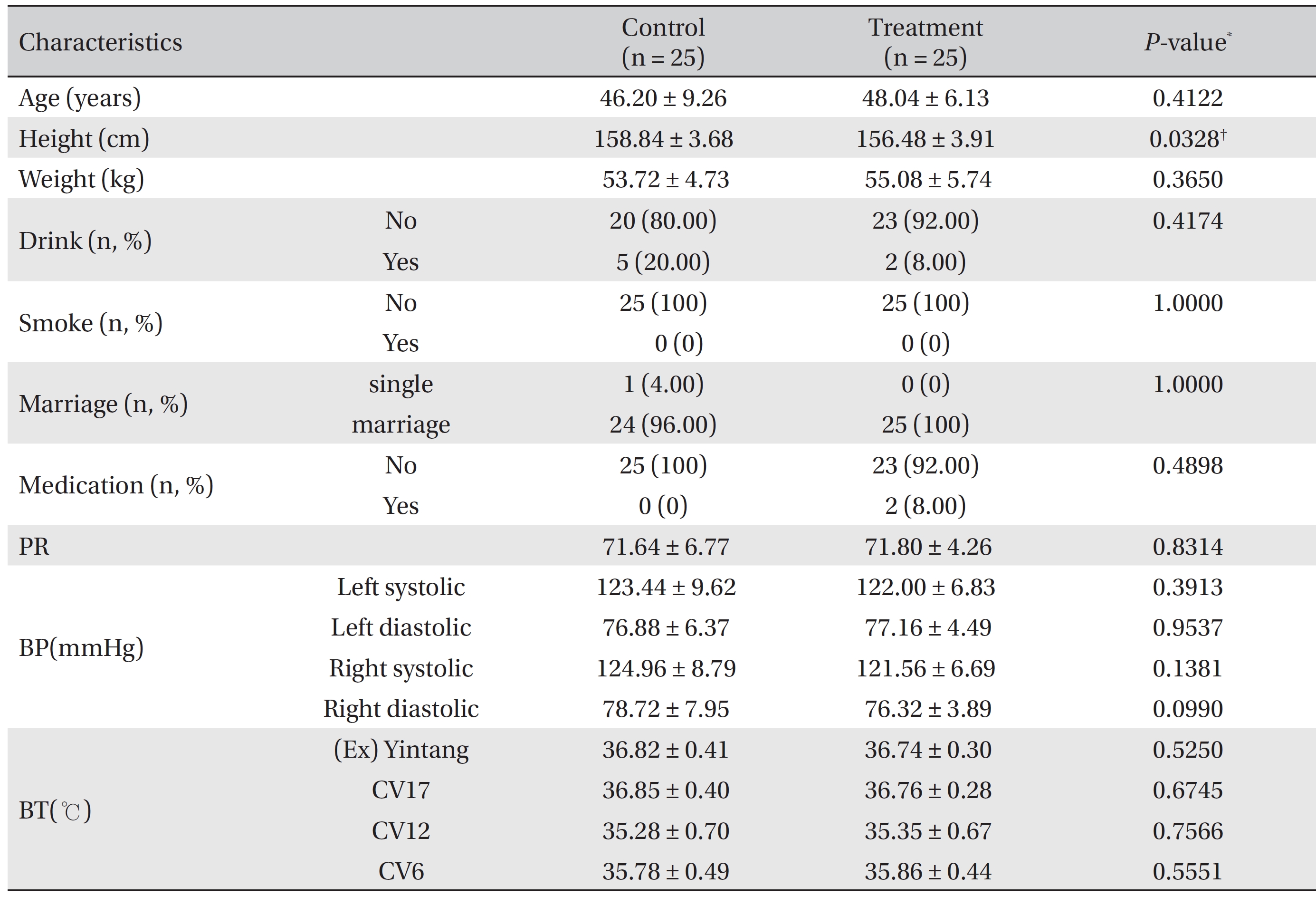
Clinical characteristics of the subjects
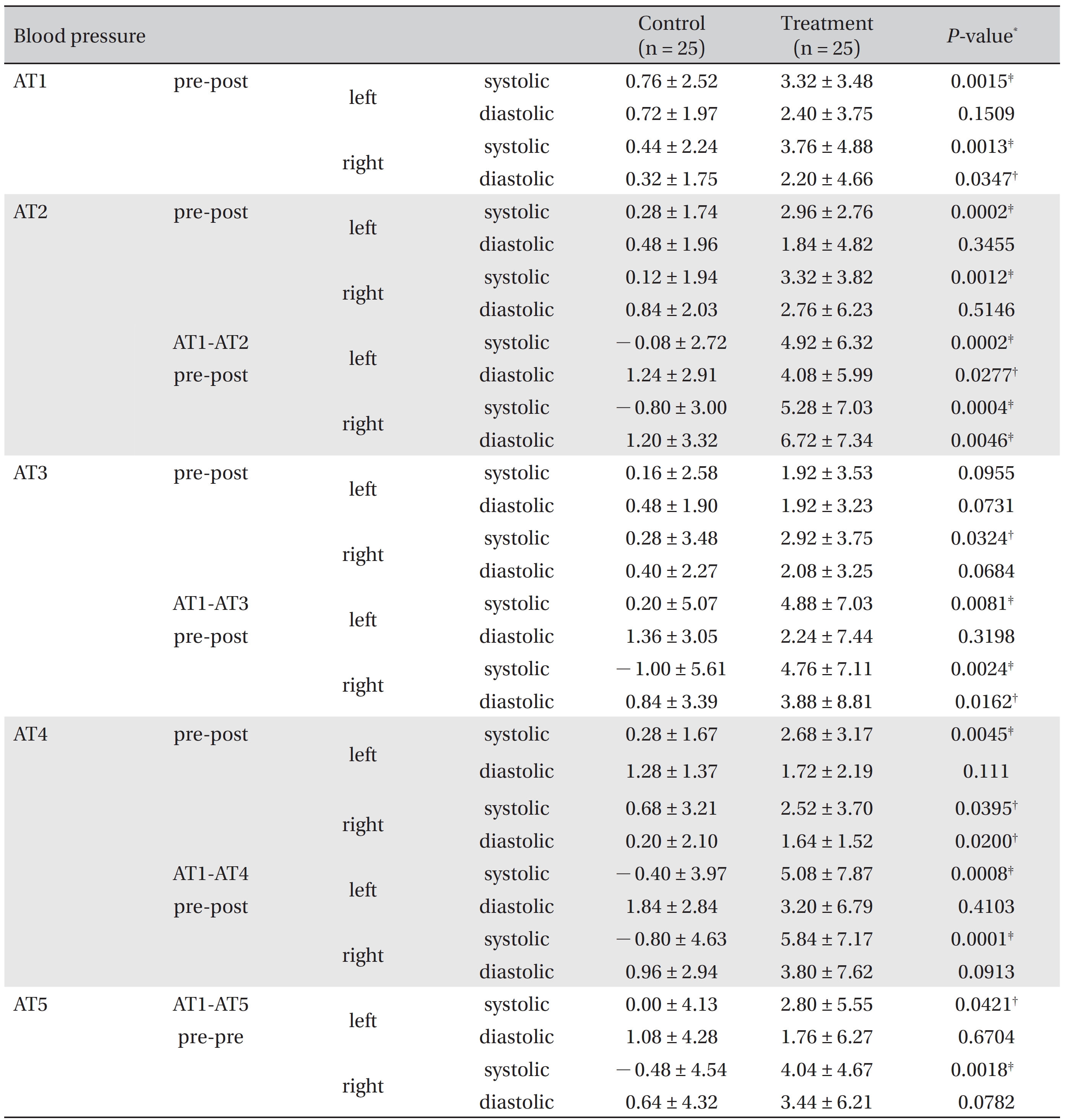
Blood pressure difference between pre-treatment and post-treatment for the control and the treatment groups
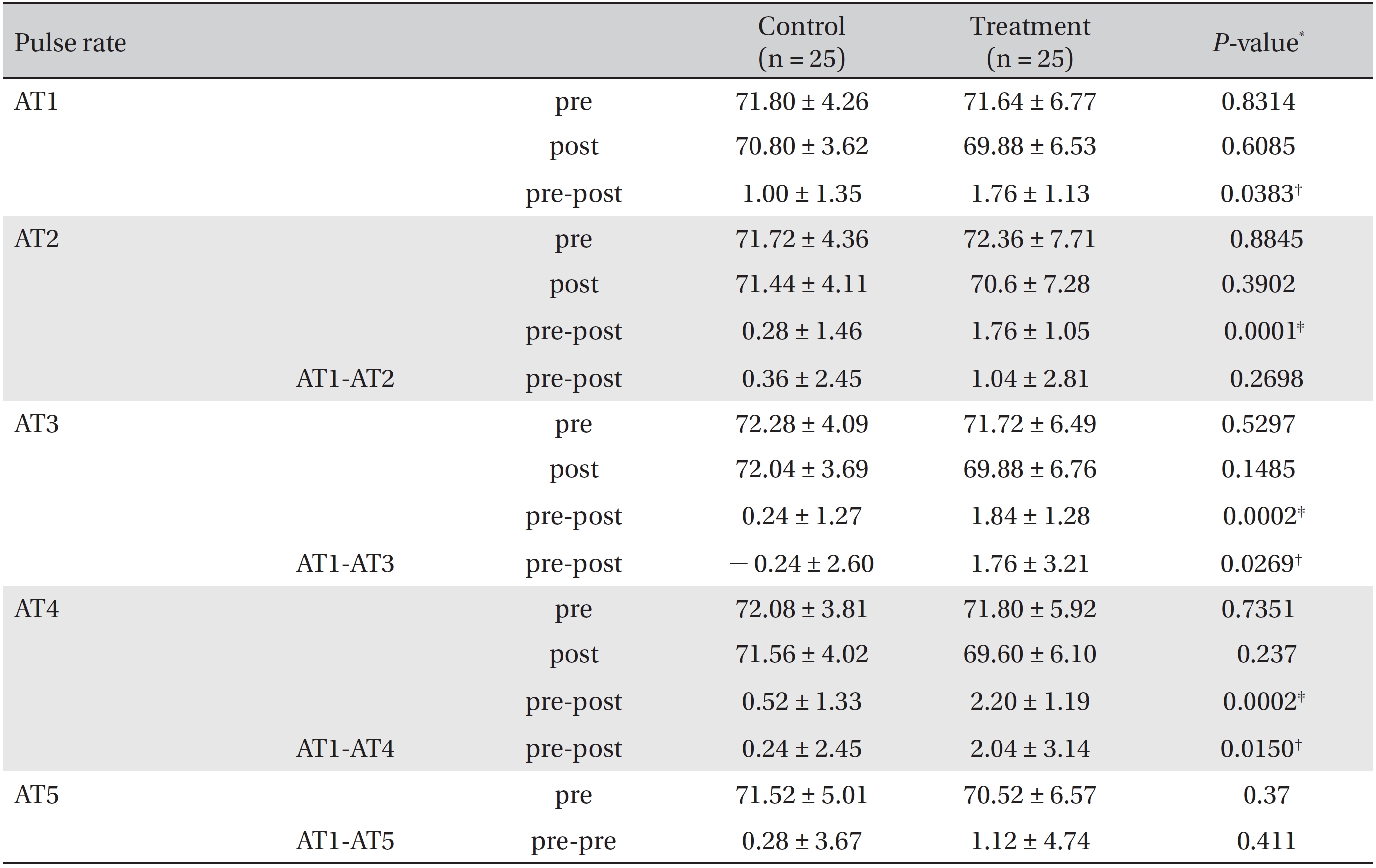
Pulse rate differences between pre-treatment and post-treatment for the control and the treatment groups
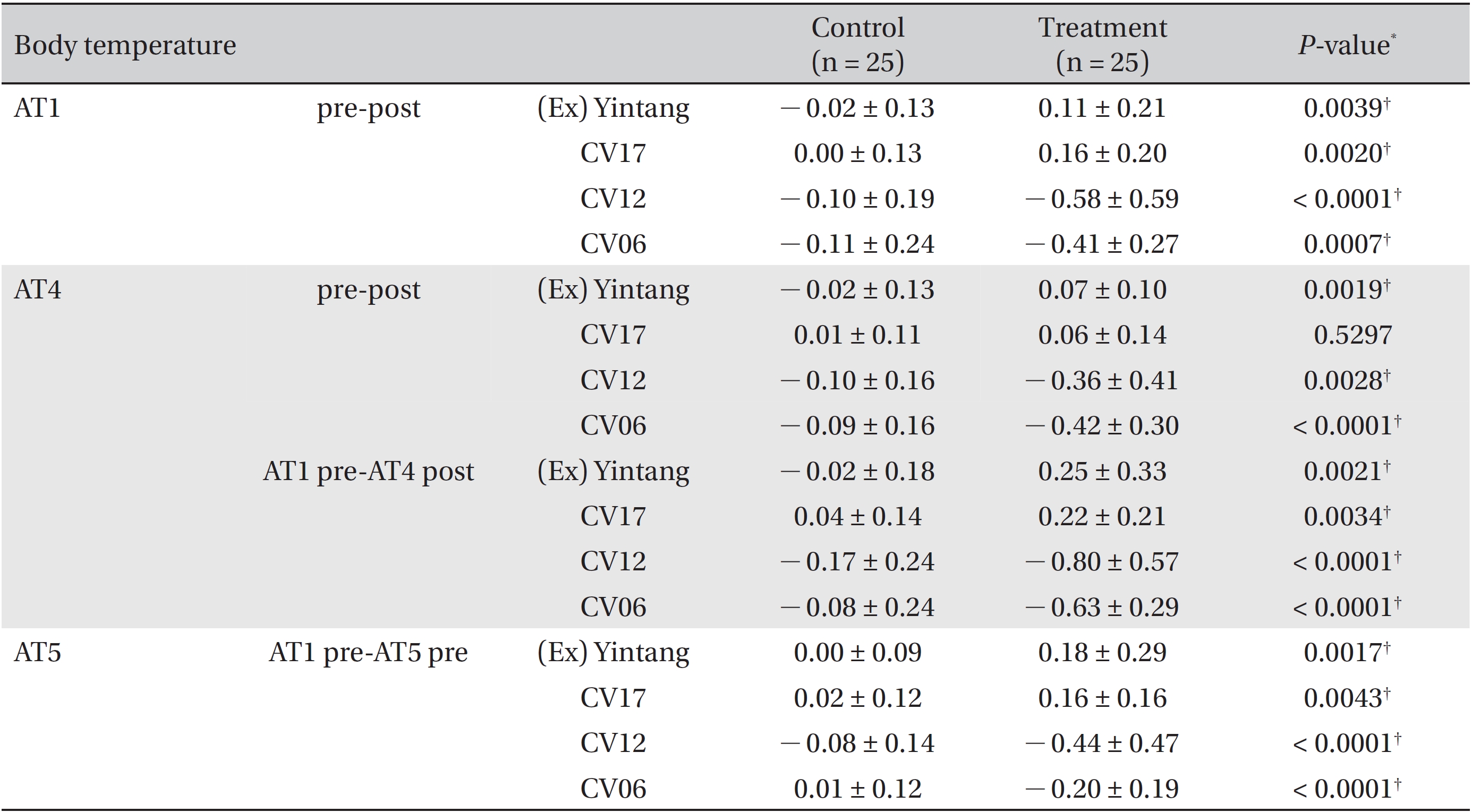
Body temperature difference between pre-treatment and post-treatment at various acupoints for the control and the treatment groups