This study was performed to estimate the effectiveness of burning acupuncture therapy (Hwachim) and sweet bee venom pharmacopuncture (S-BV pharmacopuncture) in treating lateral epicondylitis of elbow.
We selected 33 patients at first, but 13 patients were excluded due to unclear medical records. Finally, a total of 20 patients who had received treatment from January 2012 to December 2013 were included in this study; all 20 patients had undergone Hwachim for the treatment of lateral epicondylitis of elbow, and 19 of the 20 had been treated with S-BV pharmacopuncture (Korea Pharmacopuncture Institute, KPI) and transcutaneous electrical nerve stimulation (TENS) as an ancillary treatment method. The degrees of pain of the 20 patients were evaluated by using the visual analogue scale (VAS) score at their first and final visits. The Wilcoxon signed rank test and the Kruskal-Wallis test were used to compare the VAS scores statistically.
The VAS score had decreased significantly from 10.00 ± 0.00 to 4.00 ± 2.47 (P = 0.000) by the end of the treatment. No significant changes were observed based on the number of treatments (P = 0.246), the age of the patients (P = 0.810), the duration of the illness (P = 0.705), and the location of the lesion (P = 0.076).
This study suggests Hwachim and S-BV pharmacopuncture are very effective for treating lateral epicondylitis of the elbow.
Lateral epicondylitis, also known as “Tennis Elbow”, is one of the most common diseases of elbow that has, as a cardinal symptom, tenderness and pain when using the extensor muscles of wrist repetitively [1]. It usually occurs at an age from 35 to 50, but it can occur at an age from 12 to 80. Overusing the elbow joint and the forearm muscles is the major factor of lateral epicondylitis, but a sudden extreme effort or activity, such as trauma, can also cause damage to the epicondylar area [2, 3]. It is caused by an unusual contraction producing a powerful stress at the origin of the extensor carpi radialis brevis (ECRB). It can be diagnosed easily by the tenderness of the lateral epicondyle and by extending the wrist with resistance (Cozen’s test) [4].
Restricted movement, nonsteroidal anti-inflammatory drugs (NSAIDs), a gypsum cast, physical therapy, forearm strengthening exercises, a focal steroid injection and surgery are the major methods of treating lateral epicondylitis at local medical clinics [5]. The process of the disease differs from patient to patient, and much debate exists about the effects of conservative treatment and surgery. Thus, choosing an appropriate treatment is difficult.
In Korean medicine, burning acupuncture therapy (Hwachim) and sweet bee venom pharmacopuncture (S-BV pharmacopuncture) have recently been and are still being used to strengthen ligaments and to relieve pain, and some studies have reported significant results when using Hwachim and S-BV pharmacopuncture to treat lateral epicondylitis [6, 7]. We also have had good clinic experience when using Hwachim and S-BV pharmacopuncture to treat lateral epicondylitis. Thus, to evaluate the effectiveness of Hwachim and S-BV pharmacopuncture for treating lateral epicondylitis, we researched the medical records of 20 patients who had visited the Department of Acupuncture and Moxibustion Medicine, Semyung University Oriental Medicine Hospital, and who had been treated with Hwachim and S-BV pharmacopuncture from January 2012 to December 2013.
We received from the medical recorder at Semyung University Oriental Medicine Hospital a list of 33 patients who had been treated for lateral epicondylitis of the elbow by using Hwachim and S-BV pharmacopuncture at the Department of Acupuncture and Moxibustion Medicine from January 2012 to December 2013. Finally, 20 cases from that list were selected for inclusion in this research. Thirteen patients were excluded due to unclear information in their medical records. 20 patients selected from the list had severe pain on the Cozen’s test. This case report did not need approval from the Institute Review Board (IRB), Semyung University Oriental Medicine Hospital, because it was based on a chart review and was not a prospective study.
For Hwachim, the tenderness point was sterilized with an alcohol swab before treatment, and a one-time-use acupuncture needle (diameter: 0.30 mm, length: 40 mm made by Dong-Bang Acupuncture, Inc., Korea) was applied to the periosteum near the origin of the ECRB. Acupuncture was also applied to Susamli (LI10) and Gokji (LI11) in accordance with the symptoms. Before burning the needle, we put wet gauze on the lateral epicondyle to prevent burn injuries of the skin. The body of the needle was heated with a gas torch about 1 ─ 1.5 cm away from the skin until the patient felt the needle hot. After treatment, the needling point was once again sterilized with an alcohol swab.
For pharmacopuncture, 0.1 ─ 0.2 cc of S-BV pharmacopuncture (Korea Pharmacopuncture Institute, KPI) was administered at the tenderness point in 19 patients by using a 1-cc insulin syringe; 1 patient refused to undergo the pharmacopuncture treatment. Bee venom vitalizes the human immune system and has an anti-inflammation, immune cytolysis, neurotoxin effect, as well as an antibacterial and antifungal effect. There have been some significant studies about the effectiveness of using bee venom pharmacopuncture to treat lateral epicondylitis [8, 9].
Nineteen patients were treated by using a transcutaneous electrical nerve stimulator (TENS) as a physical therapy; 1 patient refused the treatment. TENS is one type of the electrotherapy that is widely using to treat diseases that cause pain, and it has an effect when it is used to treat various acute and chronic musculoskeletal and neurologic pain-causing diseases [10]. Four patients took herbal medicine granules. No other treatments were recorded in the records.
The degree of pain degree was evaluated by using the visual analogue scale (VAS) that is usually applied to estimate general pain intensity. When using that scale, patients select a number from 0 to 10 to indicate the intensity of their pain. This scale is convenient and simple to use because everyone, even a person with little education, can easily understand it [11].
SPSS 12.0 K for Windows was used to analyze the data, and the Wilcoxon signed rank test was used to compare the VAS scores before and after treatment. Also, the Kruskal-Wallis test was used to compare the VAS scores between different age groups and groups with different durations of illness. In all cases, significance was recognized for
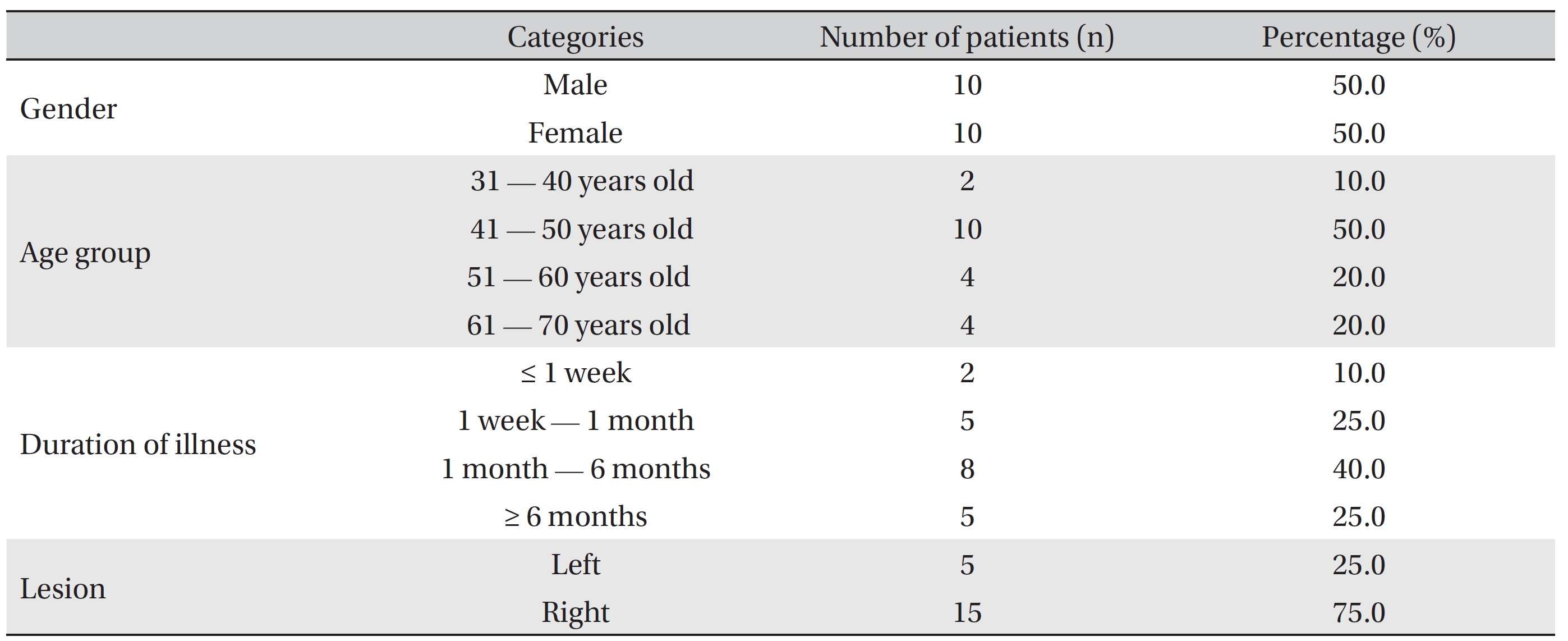
This study included 10 men and 10 women, of whom 2 were 31 ─ 40 years old, 10 were 41 ─ 50 years old, 4 were 51 ─ 60 years old, and the other 4 were 61 ─ 70 years old. Choe
Eleven patients were treated with Hwachim and S-BV pharmacopuncture 1 ─ 5 times, 5 were treated 6 ─ 10 times, and the other 4 were treated over 10 times. The VAS scores were checked at the next visits. The average of VAS score had decreased significantly from 10.00 ± 0.00 before the treatments had begun to 4.00 ± 2.47 (
The VAS scores were compared based on the numbers of treatment: after 1 ─ 5 treatments (11 patients), the average score decreased from 10.00 ± 0.00 to 4.27 ± 2.07, after 6 ─ 10 treatments (5 patients), it decreased from 10.00 ± 0.00 to 5.00 ± 2.78, and after 10 or more treatments (4 patients), it decreased from 10.00 ± 0.00 to 2.00 ± 2.61. However, the differences between these three groups were not statistically significant (
The VAS scores were also compared for four age groups. For patients 31 ─ 40 years old (n = 2), the VAS score had decreased from 10.00 ± 0.00 to 4.25 ± 1.76. For patients 41 ─ 50 years old (n = 10), it decreased from 10.00 ± 0.00 to 4.20 ± 2.44. For patients 51 ─ 60 year old (n = 4), it decreased from 10.00 ± 0.00 to 2.87 ± 2.56, and for patients 61 ─ 70 years old (n = 4), it decreased from 10.00 ± 0.00 to 4.50 ± 3.34. However, the differences between these four age groups were not statistically significant (
The VAS scores were also compared based on the duration of the illness. In the hyper-acute group (n = 2), the VAS score decreased from 10.00 ± 0.00 to 4.00 ± 0.70, in the acute stage group (n = 5), it decreased from 10.00 ± 0.00 to 5.00 ± 1.80, in the subacute group (n = 8), it decreased from 10.00 ± 0.00 to 3.18 ± 2.41, and in the chronic group (n = 5), it decreased from 10.00 ± 0.00 to 4.30 ± 3.58. However, the differences between these four groups based on the duration of the illness were not statistically significant (
[Table. 1] General Characteristics
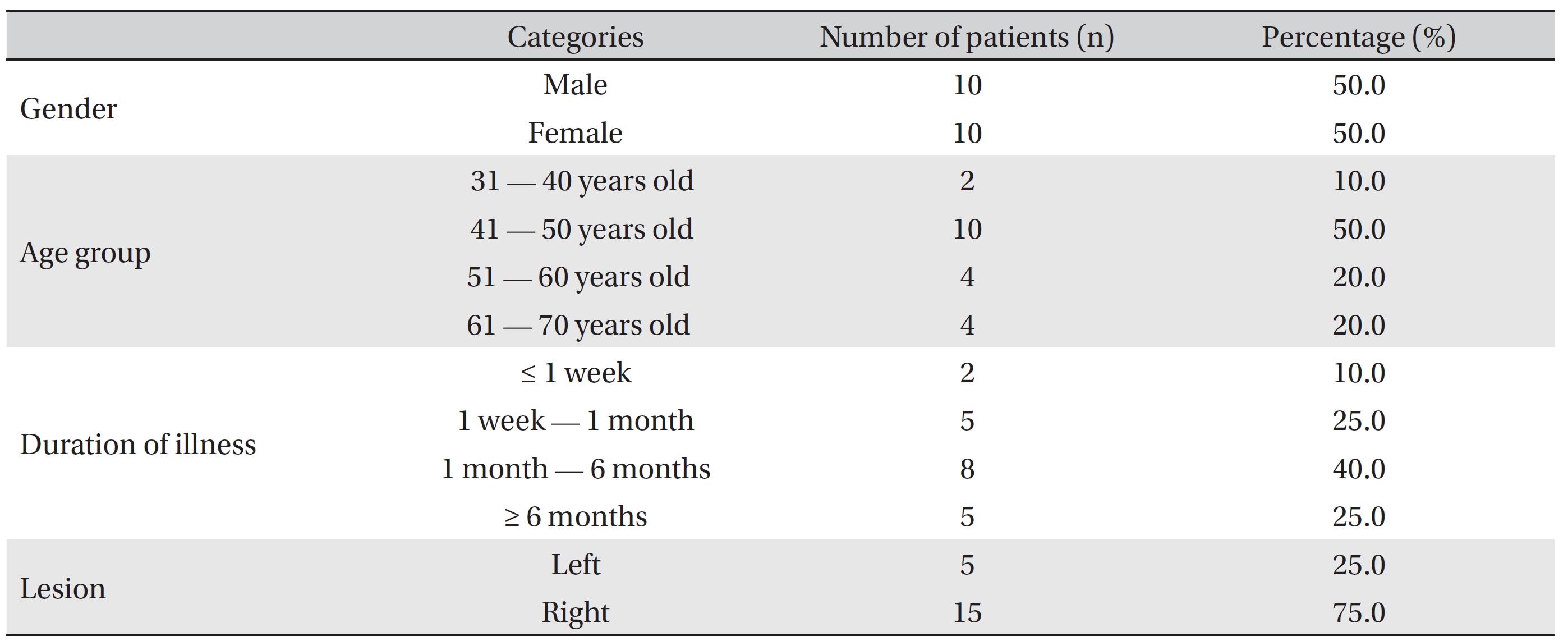
General Characteristics
[Table. 2] Comparison of the visual analogue scale (VAS) scores before and after treatment

Comparison of the visual analogue scale (VAS) scores before and after treatment
[Table. 3] Comparison of the visual analogue scale (VAS) scores based on the number of treatments

Comparison of the visual analogue scale (VAS) scores based on the number of treatments
[Table. 4] Comparison of the visual analogue scale (VAS) scores based on age

Comparison of the visual analogue scale (VAS) scores based on age
The VAS scores were also compared based on the location of the lesion. In the group experiencing left-elbow pain (n = 5), the VAS score decreased from 10.00 ± 0.00 to 2.20 ± 2.04, and in the group experiencing right-elbow pain (n = 15), it decreased from 10.00 ± 0.00 to 4.60 ± 2.36. However, the differences between these two groups based on the duration of illness the illness were not statistically significant (
[Table. 5] Comparison of the visual analogue scale (VAS) scores based on the duration of the illness

Comparison of the visual analogue scale (VAS) scores based on the duration of the illness
[Table. 6] Comparison of the visual analogue scale (VAS) scores based on the location of the lesion

Comparison of the visual analogue scale (VAS) scores based on the location of the lesion
“Tennis elbow” is popular term that was first described in 1883 as “Lawn tennis elbow” to describe a variety of painful maladies that occur in and about the elbow. Lateral epicondylitis of the elbow is currently thought to be caused by tendon overuse and failed tendon healing. Most tennis-elbow patients do not play tennis, and the condition is found almost equally in men and women. Tennis-elbow patients have pain in the lateral epicondyle of the elbow and weakness when extending the wrist and fingers. Superficial radial nerve entrapment, elbow joint lesion, osteochondritis dissecans, radiohumeral arthritis, instability of inversion, and radiating pain of the arm due to radiculopathy of the cervical spine have symptoms similar to those of lateral epicondylitis, so distinguishing lateral epicondylitis (“tennis elbow”) from other diseases is important [13].
Lateral epicondylitis of the elbow is one of the common diseases in patients with elbow pain, and it can be treated in several ways: rest, physical therapy, joint fixation, orthosis, iontophoresis, injection, etc. If elbow pain continues after treatment, surgery may be performed, depending on the patient [14]. Sufficient rest is needed in the early stage. In particular, patients have to avoid clenching their fist and strongly grabbing objects. If isometric motion is possible without pain, then isometric exercises and stretching of the extensor muscles can be done. Furthermore, if pain decreases, dumbbell exercises or other isotonic exercises may be helpful [15].
In Korean medicine, elbow pain is relevant to Bijeung, and the oldest text of Bijeung is in Huang-Di-Nei-Jing (Yellow Emperor’s Inner Canon). Bijeung is also called Yeokjeolpoong, Tongpoong after Huang-Di-Nei-Jing. In symptoms filled with bad energy (Siljeung), Huang-Di-Nei-Jing (Yellow Emperor’s Inner Canon) classified Bijeung as windy numbness and pain (Haengbi), cold numbness and pain (Tongbi), and dampy numbness and pain (Chakbi). In symptoms lacking vitality (Heojeung), the text classified Bijeung as lack of Qi and blood (Kihyulheobi), lack of Yang (Yangheobi), and lack of Yin (Eumheobi). The treatment of Bijeung is to make the dampness flow out, circulate Qi and meridians, and emit wind, cold, and dampness from human body [16, 17].
Hwachim is a treatment method that that was used in ancient times from the Huang-Di-Nei-Jing period to cure diseases by using heating acupuncture and needling in certain lesions [18]. In Huang-Di-Nei-Jing, there is a phrase that Hwachim can be used to treat muscle and bone diseases. The therapeutic range of Hwachim became wider, and it is now used to treat skin diseases, internal diseases, gynecological diseases, and ENT diseases. Now, it is also used in many different fields: It can make the ligament stronger by causing an inflammatory reaction in the ligament, boost Yangqi in the human body, circulate meridians and meridian points, and expel bad energy [19]. Traditionally, in Hwachim, the acupuncturist heated the needle before applying acupuncture, but nowadays the acupuncturist heats the needle after applying acupuncture to lesion. The latter is more effective in avoiding injury to dense connective tissues. Hwachim can stimulate heat that is deeper than moxibustion, and hotter than a warm needle (Onchim). Also, the acupuncturist can control the temperature of the needle by using the power of the heating system [20].
All of the patients in this study had pain and tenderness in the lateral epicondyle of the elbow, and all had a positive reaction on Cozen’s test. Most of them also experienced weakness when grasping an object or pain when grabbing and lifting an object. Thus, we applied Hwachim and S-BV pharmacopuncture to the origin of the ECRB several times. The overall VAS score decreased from 10.00 ± 0.00 before treatment to 4.00 ± 2.47 (Table 2) after treatment.
In a study, Park
In this case study, we applied Hwachim in 20 patients, so the results of this study should be meaningful for treating lateral epicondylitis with burning acupuncture therapy. Finally, although we can conclude that the use of Hwachim and S-BV pharmacopuncture is effective in treating lateral epicondylitis, this study has several limitations: The number of cases was insufficient, and other treatments like TENS were also done simultaneously. Moreover, we plan to study the dependence of the reduction of pain on the duration of the treatment more. The mechanism of Hwachim has not been clearly proven to be effective until now, so more cases and continuous study are needed before Hwachim can become a general treatment method.
The conclusions of this study involving combined Hwachim and S-BV pharmacopuncture treatment in 20 patients with lateral epicondylitis of the elbow are as follows: The VAS score decreased significantly from 10.00 ± 0.00 before to 4.00 ± 2.47 (