The purpose of this study is to determine the type-2 diabetes risk status of the individuals applying to the internal diseases outpatient clinic and the affecting factors. This descriptive study was conducted on 500 individuals who applied to the internal diseases department of a hospital in Ordu Turkey, between May and June 2010 without diabetes diagnosis. The questionnaire form and Type 2 Diabetes Risk Assessment Form are used to collect the data. For the evaluation of data; independent samples t-test and One-Way Anova are used to evaluate the data. It is determined that the type-2 diabetes risk an score of the individuals participating in the study is 10.4 ± 5.5 and 32.4% of them have low type-2 diabetes risk score, 26.6% have slightly elevated score, 18% have moderate score, 16.6% have high and 6.4% have very high type-2 diabetes risk score. It is found that the type-2 diabetes risk mean score of the women participating in the study who are adults, are married, have low education level, are unemployed, are non-smoker, do not drink alcohol and do not have any information about type-2 diabetes is statistically significantly high (p < 0.05). It is determined that 16.6% of the individuals participating in the study have high type-2 diabetes risk and 6.4% have very high type-2 diabetes risk.
Diabetes is a metabolic syndrome which is characterized with chronic hyperglycemia, causing the organism to create failures in carbonhydrate, protein and fat metabolism because of insulin deficiency or the defects in the insulin action (Satman et al., 2009). Type-2 diabetes constitutes more than 90% of the diabetes cases getting the diagnosis throughout the world (Garduño-Diaz and Khokhar, 2007; Guler et al., 2011) type-2 diabetes is a global health crisis which threatens the economies of all the countries, especially the developing countries (Alberti et al., 2007; Hu, 2011; Mayor, 2007; Wu et al., 2011).
It is estimated that there are 285 million diabetic patients all around the world and diabetes is developing in seven million people every year and this number is anticipated to reach 438 million in 2030 (Hu, 2011). As of 2010, it is specified that approximately 26 million working-age American people have type-2 diabetes (Anderson et al., 2012). In China, the type-2 diabetes prevalence in 1980 was less than 1% and this ratio is 10% in 2008 (Hu, 2011). It is specified that type-2 diabetes incidence is rapidly growing in Turkey and the incidence is 300 thousand throughout the country and diabetes frequency in adults has reached 13.7% (Guler et al., 2011; Onat et al., 2006).
Diabetes causes severe organ damages and deaths (Alberti et al., 2007; Grundy, 2012; Thomas et al., 2012). Half of the renal function disorders have been caused by type-2 diabetes and diabetic renal disease is in the first place within the terminal stage kidney diseases (Thomas et al., 2012). Around the world, it is specified that approximately 93 million people have diabetic retinopathy, 17 million people have advanced diabetic retinopathy, 21 million people have diabetic macular edema and 28 million people have diabetic retinopathy which causes visual defects (Yau et al., 2012). Type-2 diabetes causes coronary artery diseases, cardiac insufficiencies, strokes and deaths (Alberti, 2007; Cobble and Frederich, 2012). It is indicated that a second amputation ratio in a diabetic foot is 18% (Borkosky and Roukis, 2012).
Diabetes is a very-high cost disease (Alberti et al., 2007; Anderson et al., 2012; Waugh et al., 2007). The total expense made for diabetics in Turkey is 1.1 billion dollars and every 10% increase in the complication frequency causes an increase of 180 - 190 million in the expenses per year (Satman et al., 2009).
Regarding to fighting with type-2 diabetes and the risk factors, policies are developed in all around the world and national action plans are prepared. The life style changes to be done for preventing type-2 diabetes are accepted as a cheap and easy method which can be applied socially (Alberti et al., 2007; Satman et al., 2009).
In order to prevent type-2 diabetes, at first the risk factors should be determined (Alberti et al., 2007; Kodama et al., 2012; Onat, 2007). Gender, age and ethnicity, family history, living style, smoking, dyslipidemia, hypertension, waist circumference and obesity are among the important risk factors (Alberti et al., 2007; Hu, 2011; Onat et al., 2006; Salopuro, 2011). For diabetes, it is important to determine the individuals at risk without the disease symptoms in terms of maintaining and improving the health (Garduño-Diaz and Khokhar, 2007; Shi, 2011). Since the people-at-risk can be identified at the prediabetic stage of impaired glucose tolerance, it can be possible to prevent diabetes and its complications by taking early stage precautions (Alberti et al., 2007; Onat et al., 2007).
In the comprehensive studies conducted on the possibility of preventing or delaying type-2 diabetes; as well as the pharmacological agents, the success of life style changes is shown. It is demonstrated that type-2 diabetes may be prevented to a large extent such as 58% in the ethnic groups especially prone to diabetes with nutrition, exercise and body weight control (Alberti et al., 2007).
It is stated that the lifetime of patients will extend, the living quality will increase and economic burden will decrease by preventing or delaying type-2 diabetes (Alberti et al., 2007; Mayor, 2007). In the type-2 diabetes prevention plan, at first the high-risk groups should be determined and then the whole society should be targeted. For determining the high-risk groups in type-2 diabetes, practitioners, nurses and pharmacists may take in charge (Alberti et al., 2007; Mayor, 2007). The nurse, one of the important members of the medical team, can give a professional support to prevent type-2 diabetes by using research, training and consultancy roles. The nurse can determine the risk groups and effective factors for type-2 diabetes and give training and consultancy to this group and make a significant contribution to the prevention of type-2 diabetes.
The purpose of this study is to evaluate type-2 diabetes risk status and affecting factors of the individuals who applied to the internal diseases outpatient clinic.
The study was conducted on 500 individuals who applied to the Internal Diseases outpatient clinic of a hospital in Ordu (Turkey) between May and June 2010. During this period, 572 individuals were admitted to the internal medicine outpatient clinic. 72 patients did not provide the research inclusion criteria (15 patients refused to participate in the study and 57 patients were diabetics) were excluded from the study. The 18 year-old and older people who accepted to participate in the study and had no diabetes disease were included in the study.
An questionnaire form and type-2 diabetes Risk Assessment Form are used to collect data of the study. In the questionnaire form; there are 11 questions in total specifying the sociodemographic properties, smoking status, alcohol usage status and knowledge about type-2 diabetes of the participants. In order to determine the Type 2 Diabetes Risk, a Type 2 Diabetes Risk Evaluation Form created in parallel to “FINDRISK Risk Questionnaire”, which is commonly used in our country and referred by The Society of Endocrinology and Metabolism of Turkey, was used. This form has totally 8 questions including the age, body mass index, waist circumference, exercise status, fruit and vegetable consumption, elevation of the blood pressure, whether or not the blood glucose level is high previously and the diabetes presence in the family for genetic transfer. If the total score in the form is 20 and more, this means there is a very high risk, 15 - 19 score is high, 12 - 14 score is moderate, 7 - 11 score is slightly elevated and score lower than 7 is low risk.
Independent samples t-test and One-Way Anova were used in order to evaluate data.
Ethical Considerations: The participants were informed about the study and their consent was obtained. Also a written permission was taken from the institution where the study was conducted.
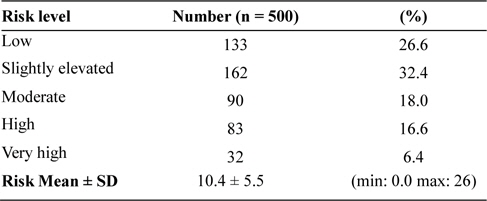
It was determined that the type-2 diabetes risk mean score of the individuals participating in the study is 10.4 ± 5.5 and 32.4% of them had low, 26.6% had slightly elevated, 18% had moderate, 16.6% had high and 6.4% had very high type-2 diabetes risk (Table 1).
[Table 1.] Type 2 Diabetes Risk Percentages Distribution and Risk Mean of the participants
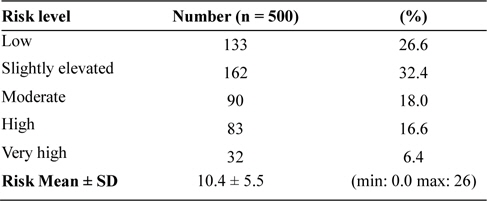
Type 2 Diabetes Risk Percentages Distribution and Risk Mean of the participants
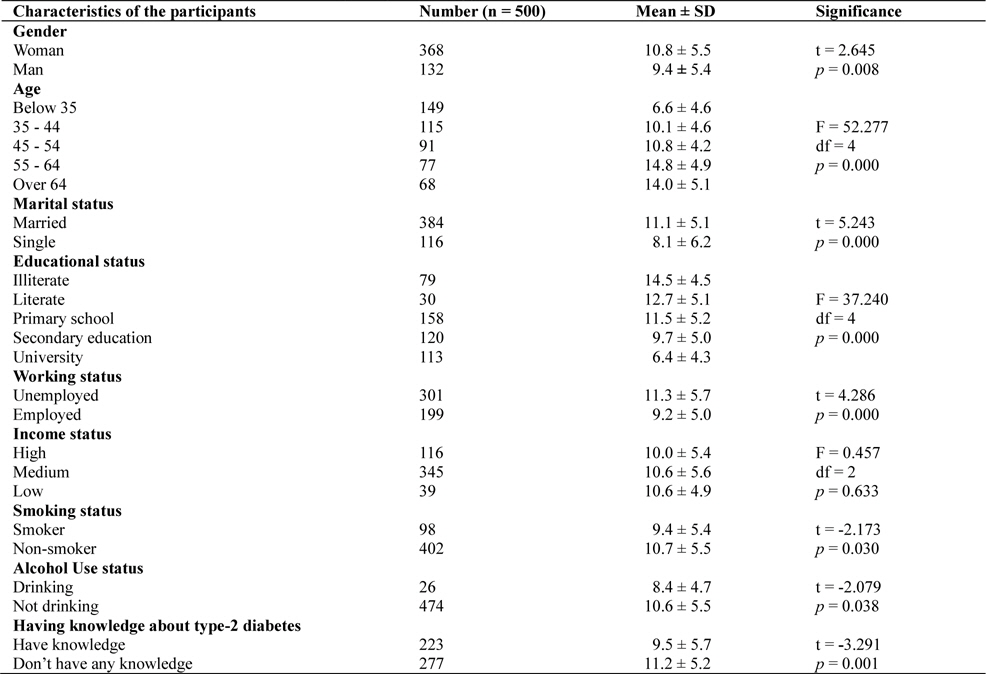
It was determined that the type-2 diabetes risk mean score of women was significantly higher than those of men (
[Table 2.] Comparison of the characteristics of the participants and Type 2 Diabetes Risk Scores
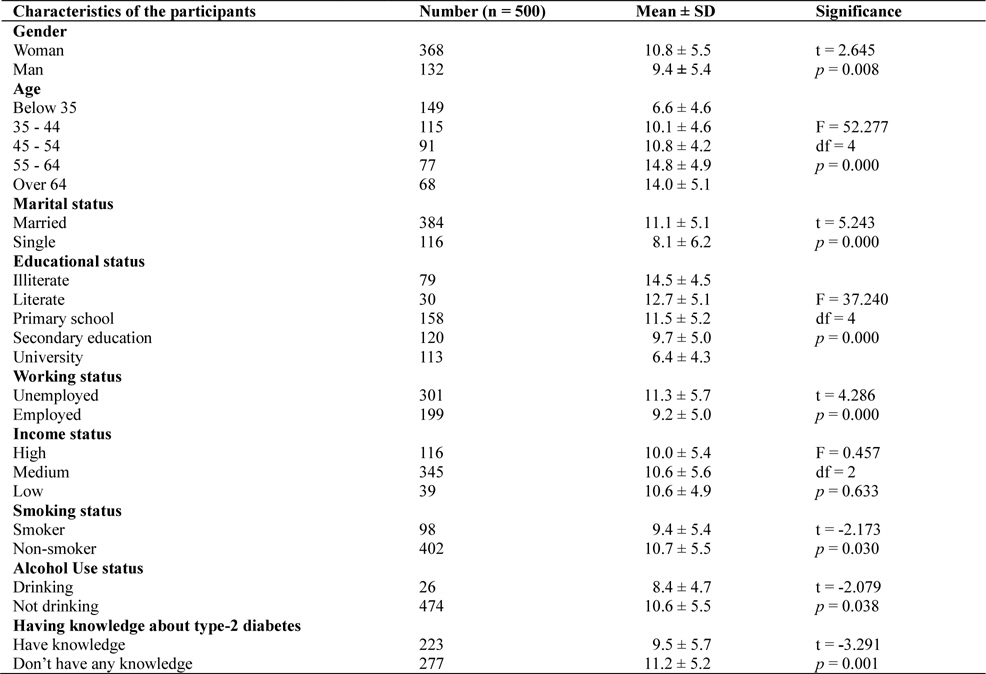
Comparison of the characteristics of the participants and Type 2 Diabetes Risk Scores
In type-2 diabetes prevention plan, it is specified that the high risk groups should be obtained in diabetes prevention program (Alberti et al., 2007). It is recommended for the high risk people in type-2 diabetes to make changes in their life styles at first. In life style adjustments, it is indicated that weight control, healthy nutrition and regular physical exercise will prevent the development of type-2 diabetes. If the life style changes are unsuccessful, drugs should be started to be taken (Mayor, 2007). 16.6% of the individuals participating in the study had high risk and 6.4% had very high risk.
Various studies concluded that no difference is present between the genders for type-2 diabetes (Imbeault et al., 2011; Sacerdote et al., 2012). Diabetes frequency is lower in men than women and it is indicated that there is no significant difference between the genders (Guler et al., 2011). In Turkey, type-2 diabetes is also common in men as much as in women (Onat, 2011). Contrary to the literature information, it is found that type-2 diabetes risk in the women participating in the study is significantly higher in comparison to the men.
It is indicated that glucose intolerance, insulin resistance and type-2 diabetes development increase together with the age and type-2 diabetes has a peak value between 60 and 74 (Gong and Muzumdar, 2012). As the age increases; type-2 diabetes frequency also increases (Alberti et al., 2007; Gunasekaran et al., 2011). It is determined that type-2 diabetes risk has significantly increased with the ages of the participants in accordance with the literature.
It is specified that there is an inverse relationship between the education status and diabetes incidence (Robbins et al., 2005). Low educational level causes high risk for type-2 diabetes (Imbeault et al., 2011). It is determined that there is a relationship between type-2 diabetes and low educational status (Agardh et al., 2011). Pursuant to the literature, when the educational levels of the participants decrease, type-2 diabetes risk increases significantly.
It is found that diabetes incidence in working women is lower however there is no relationship between the diabetes incidence and working status for men (Robbins et al., 2005).
There is an inverse relationship between the working status and type-2 diabetes (Agardh et al., 2011). In our study, it is determined that type-2 diabetes risk is significantly lower for employed participants.
It is pointed out that type-2 diabetes is commonly seen among the poor people and 2/3 of the diabetes patients all around the world live in low and medium-income countries (Hu, 2011). It is specified that there is an inverse relationship between the income status and diabetes incidence (Robbins et al., 2005). Socio-economic status insufficiency may be a risk factor for type-2 diabetes (Sacerdote et al., 2012). It is determined that there is a relationship between low socioeconomic status and type-2 diabetes (Agardh et al., 2011). Type-2 diabetes risk is more in the participants with low and medium income; however the increase is not significant.
It is determined that the relationship between smoking and type-2 diabetes is not clear (Sacerdote et al., 2012). It is indicated that smoking is an independent risk factor for type-2 diabetes and type-2 diabetes development risk increases in smokers (Hu, 2011; Willi et al., 2007). It is specified that smoking may protect the women smoking a lot (11 or more per day) from being overweight and it may be preventive against diabetes and metabolic syndrome in the future (Onat et al., 2007). It is determined that type-2 diabetes risk in smoking people is significantly low.
Although conducted studies specified that little alcohol usage may decrease type-2 diabetes risk, the clinical data does not support the recommendation of alcohol consumption for the individuals with diabetes risk (Satman et al., 2009). It is indicated that low and moderate level of alcohol consumption decreases type-2 diabetes risk (Hu, 2011). It is found that the participants taking alcohol have significantly low type-2 diabetes risk.
CONCLUSIONS AND RECOMMENDATIONS
As a result of the study, it is determined that the type-2 diabetes risk mean score of the individuals is 10.4 ± 5.5 and 32.4% had low, 26.6% had slightly-elevated, 18% had moderate, 16.6% had high and 6.4% had very high type-2 diabetes risk. It is found that the type-2 diabetes risk was higher in women who are adults, are married, have low education level, do not work, do not smoke, do not drink alcohol and do not have any knowledge about type-2 diabetes.
At the end of this research, it is recommended: to take the individuals with high and very high type-2 diabetes risk scores to a diabetes prevention program, to prioritize women, old aged participants, married participants, unemployed participants and those having low educational level in the Type 2 Diabetesprevention program, and to have the nurses use their educational roles actively and efficiently about preventing type 2 diabetes.