To investigate the minimum near-infrared ray intensity required (quantifiable threshold value) for consistent measurements of axial length (AL) using partial coherence interferometry (PCI), we attached two polarizing lenses (PL) to two types of PCI (IOLmaster, ALscan). The near-infrared ray intensity of PCI was modified by rotating the axis of one PL at intervals of 5 degrees. The right eye of each volunteer was measured three times and the AL and signal-to-noise ratio (SNR) was recorded five times for each measurement. Reduction of light intensity was theoretically estimated using Malus’ Law. AL was measured consistently with both IOLmaster and ALscan until they reached 55 degrees (1.33 % of intensity) and 60 degrees (0.77%), respectively (P = 0.343, Log-rank test). In contrast, SNR decreased as light intensity decreased. In addition, to analyze media opacities that precluded measurement of AL, we retrospectively reviewed the medical records of patients unmeasurable by PCI (ALscan) from May to November 2013. Thirty-eight of 473 eyes (8.0%) could not be measured using ALscan due to media opacities, such as severe posterior subcapsular cataract (PSC, 11 eyes), hypermature cataract (9 eyes), and vitreous hemorrhage (18 eyes). The mean grades of vitreous haze and PSC were 7.72 ± 0.96 and 4.45 ± 1.04, respectively. In conclusion, up to 0.77−1.33% of near-infrared rays decreased, and AL could be measured consistently.
Accurate measurement of ocular axial length (AL) is the most important step for accurate intraocular lens (IOL) power calculations. [1] Accordingly, partial coherence interferometry (PCI) is commonly used to measure ocular AL. PCI provides more accurate, reproducible, and non-contact measurements of ocular AL compared with conventional contact ultrasound methods. [2] PCI uses a laser diode (LD) in the near-infrared spectrum (780 nm) with a high resolution (12 μm) and precision (0.3-10 μm) along the fixation line of an eye.[3, 4] The LD in PCI produces coaxial dual beams and mirrors split them into two equal coaxial beams which reflect the beams into the eye (Fig. 1).[5, 6] The measurement mirror moves with constant speed and superimposes the reflected beams from the retina onto the delayed beams from the cornea. [5, 6] Then the interference signal is detected and the displacement of the mirror can be precisely obtained. [5, 6] The delay of dual beam components equals the axial length. [5, 6]
However, PCI is less useful in measuring AL in eyes with severe media opacity, especially due to posterior subcapsular cataracts (PSC). It is reported that the failure rate of AL measurement using PCI was 4.7-36.6% because of dense nuclear sclerosis, PSC, macular pathology, vitreous opacity, and other similar disorders. [7-10] These failures could arise from using devices from different manufacturers, different software versions, differences in regional or hospital/practice settings, etc. [10]
Related to this, unsuccessful measurements of PCI in eyes with severe media opacities meant that the near-infrared light beam centered at 780 nm could not penetrate the opacities. Although we commonly knew the severities of opacity using the Lens Opacities Classification System III (LOCS III) or other grading systems, no studies have assessed the minimum near-infrared ray intensity required for constant PCI measurements of AL. Some studies revealed that increased cataract density could affect the measurements of ocular AL and postoperative refractive outcomes. [11, 12] However, studies were also carried out including eyes that were successfully measured.
We therefore measured the minimum near-infrared ray intensity required for consistent measurements of AL to quantify a threshold value at which the measurement of AL became unreliable for PCIs. We also analyzed media opacities in patients with media opacities that precluded measurement using PCI.
2.1. Measurement of the Minimum Near-infrared Ray Intensity
Two commercially available types of PCI, IOLmaster 500 (Carl Zeiss Meditec, Dublin, CA) and ALscan (Nidek Technologies, Gamagori, Japan) were used. Two polarizing lenses (PL, Kenko Tokina, Tokyo, Japan) were attached to the measuring part of the PCI. The near-infrared ray intensity of the PCI was modified by rotating the axis of one PL at intervals of 5 degrees. AL and signal-to-noise ratio (SNR) were recorded five times for each measurement and were provided by each PCI. The right eyes of healthy volunteers with no previous ocular disease were measured three times. Reduction of light intensity was theoretically estimated using Malus’ Law. The double path nature of the device which attenuated the light twice was considered to calculate the reduction of light intensity. The minimum near-infrared ray intensity was recorded as the intensity of the near-infrared ray that was calculated from the maximum angle between the two PLs offering constant measurements of ocular AL. The difference of AL according to the attenuation of light intensity was defined as the subtraction of AL in the uncrossed state from the crossed states. The percentage of SNR was defined as the percentage of the measured SNR in the crossed state over the SNR in the uncrossed state.
2.2. Analysis of Media Opacities Precluding Successful Measurement using PCI
We retrospectively reviewed the medical records of patients unmeasurable by ALscan from May to November 2013. The following parameters were analyzed: preoperative visual acuity (logarithm of the minimum angle of resolution, logMAR); lens opacity graded as LOCS III [13]; and vitreous opacity graded using the vitreous haze scale for photographic grading of vitreous haze in uveitis from 0 (none) to 8, with approximately 0.3 log step between each step. [14]
Data are presented as means ± standard deviations, unless otherwise specified in the text. Differences were analyzed with PASW software version 18.0 (SPSS, Chicago, IL). Measurability of PCI was compared using Kaplan-Meier survival curves and the log-rank test. SNR was analyzed using linear regression. The Mann-Whitney
3.1. Measurement of the Minimum Near-infrared Ray Intensity
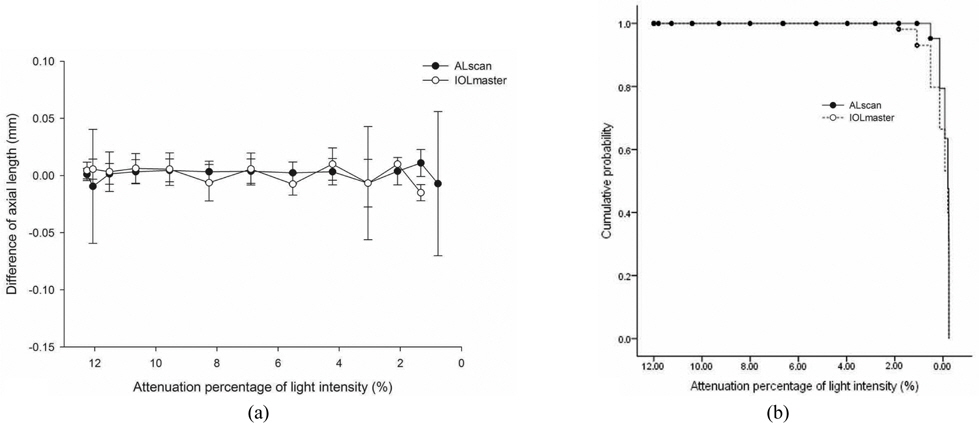
Seven right eyes from seven subjects were recruited. The average age was 34.0 ± 6.2 years and the average AL was 25.21 ± 1.69 mm with ALscan and 25.20 ± 1.68 mm with IOLmaster. AL was measured consistently with both ALscan and IOLmaster, until they reached 60 degrees (0.77% of intensity) and 55 degrees (1.33% of intensity), respectively. The differences of AL retained near zero, which meant consistent measurements of AL were done until they reached 0.77 to 1.33% of near-infrared ray intensity of the PCI (Fig. 2A). There were some missing values due to an inability to measure AL under 1.33% of intensity using IOLmaster. However, there were no statistical differences in the measurability between the two types of PCI (Fig. 2B,
3.2. Analysis of Media Opacities Precluding Successful Measurement using PCI
Measurement data of 473 eyes in 237 patients using ALscan were reviewed. AL could not be measured in 38 of 473 eyes (failure rate, 8.03%). The mean age of the patients was 62.87 ± 13.36 years and the average of the best corrected visual acuity (BCVA, logMAR) was 2.12 ± 0.96. Media opacities causing failure of AL measurements were vitreous hemorrhage (VH, 18 eyes), severe PSC (11 eyes), and hypermature cataract (9 eyes). The mean grades of vitreous haze and PSC (LOCS III) were 7.72 ± 0.96 and 4.45 ± 1.04, respectively. There were no statistical differences in age and gender among the different causes for opacities (Table 1). However, the visual acuity in eyes with dense PSC was better than that in eyes with other opacity causes (
[TABLE 1.] Preoperative data of patients who failed to be measured

Preoperative data of patients who failed to be measured
In previous studies, the failure rates using PCI and the precludable opacities were reported as 4.7-36.6%. [7-10, 15] However, there were no reports with the objective of comparing the minimum intensity of opacity that could offer successful measurements as a threshold value to measure the AL accurately. Our results showed that AL could be measured consistently when up to 0.77-1.33% of near-infrared rays passed through. We used two easily obtainable PLs and Malus’ Law, which is one of the well-known principles describing the relationship between polarization and the intensity of the light that passes through an optical material. [16] Because we used inexpensive and easily obtainable materials, the measurability test could be easily reproduced. We used Malus’ Law and theoretically assumed the intensity of near-infrared rays that passed through, which might overestimate the minimum intensity of light required. However, it was in good agreement with measured data when the incident light is partially polarized. [17]
Another consideration was the corneal birefringence that might affect the intensity when rotating the axis of the attached PL. [18-20] The cornea is the major birefringent ocular structure, and corneal birefringence varies depending on the location and the orientation. [18] To rule out the effect of orientational variation of corneal birefringence, we also measured AL while rotating one PL at intervals of 5 degrees. There were no differences in measuring AL using PCI according to the axis of the PL from 0 to 180 degrees (data not shown). Although conducting measurements three times per axis might mask any possible minimal differences, these differences would be meaningless in the clinical use of PCI.
Successful measurements could be obtained with up to 0.77-1.33% intensity of the near-infrared rays. Measurements obtained using two different PCIs showed similar results. Figure 2 shows that the differences of AL between the AL in the uncrossed state and that in the crossed states retained near zero which means consistent measurements of AL until they reached 0.77 to 1.33% of near-infrared ray intensity of the PCI. We considered the minimum light intensity with reliable data of AL as a threshold value of measurement. This is the first report to investigate the measurability of PCI with a concept of measurement threshold value. Clinically, this meant that the patients with failed AL measurements could have opacities which blocked or scattered more than 99% of the light at the center of the optical axis of the eye. IOLmaster could not measure under an intensity of 1.33%, which seemed to be higher than those using ALscan 0.77%. However, there were no statistically significant differences between the two PCIs in the measurability using Kaplan-Meier survival curves and in the differences of AL according to the attenuation of light intensity. The SNRs using both PCIs decreased as light intensity decreased, as expected. The measured range of SNR was different between two PCIs. The different range of SNR would come from the use of different algorithms, devices from different manufacturers, etc. Therefore, we also analyzed the percentage of SNR according to the attenuation of light intensity and they showed significant correlations.
One of the commercially available PCIs, ALscan was recently introduced by Nidek Technologies, and there are no reports of the failure rate using this PCI. Our results show a failure rate of 8.03%. Although patients with vitreous hemorrhage or severe cataract visited our hospital as a tertiary referral center in our consolidated city-county region, the failure rate was not as high when compared to previous reports using IOLmaster. [7-10] Because of the limitations of retrospective chart review, we could not obtain repeated measurements of AL using two PCIs, which could have shown whether measurability between two PCIs might differ or not,in clinical aspects. However, we inferred similar results between the two PCIs from our objective measurements of minimum intensity that offered consistent AL.
We revealed the minimum intensity of infrared ray (0.77-1.33%) for consistent measurement of AL using PCI. This could be considered as a quantifiable threshold of AL measurement. This was the first report to investigate the quantifiable measurability of PCI with a concept of measurement threshold. As a clinical aspect, this study showed that the patients with failed AL measurements could have opacities which blocked or scattered more than 99% of the light at the center of the optical axis of the eye. We also reported the failure rate of a recently introduced PCI. Though there were differences between visible and infrared light, we expect that our results will provide some insight into investigating the visual impacts of opacities in an eye according to their density and location.