Peripheral facial paralysis is a disease that is found in 20 cases per 100,000 people per year [1], and that has symptoms such as postauricular pain, dysgeusia, hyperacusis, lacrimation, and facial muscular paralysis on the affected side. Types of the disease mostly include Bell's palsy, Ramsay Hunt’s syndrome, cerebellopontine angle tumors, basilar skull fractures, and thyroiditis; Bell's palsy, which is related to inflammation or dilation of the facial canal or the stylomastoid foramen without adistinct structural lesion accounts for 90% of the cases [2].
Bell’s palsy is generally caused by exposure to coldness, overwork, mental shock, and stress without causative disorders or trauma [3]. Its treatments are roughly divided into drug therapy and surgery [3]. A majority of scholars support drug therapy with steroids and vasodilators to treat Bell’s palsy, and the administration of steroids [4] accompanied by physiotherapy and facial exercise is a method of treatment whose effects have been evidenced by several studies. However, loss of the beauty of balance and functional faults caused by facial paralysis may significantly affect the patients mentally and socially [5]. Oriental medicine uses acupuncture [6-9] and herbal drug therapy, pharmacopuncture, and Oriental medicine physiotherapy to treat the disease. Studies of pharmacopuncture related to peripheral facial paralysis have focused
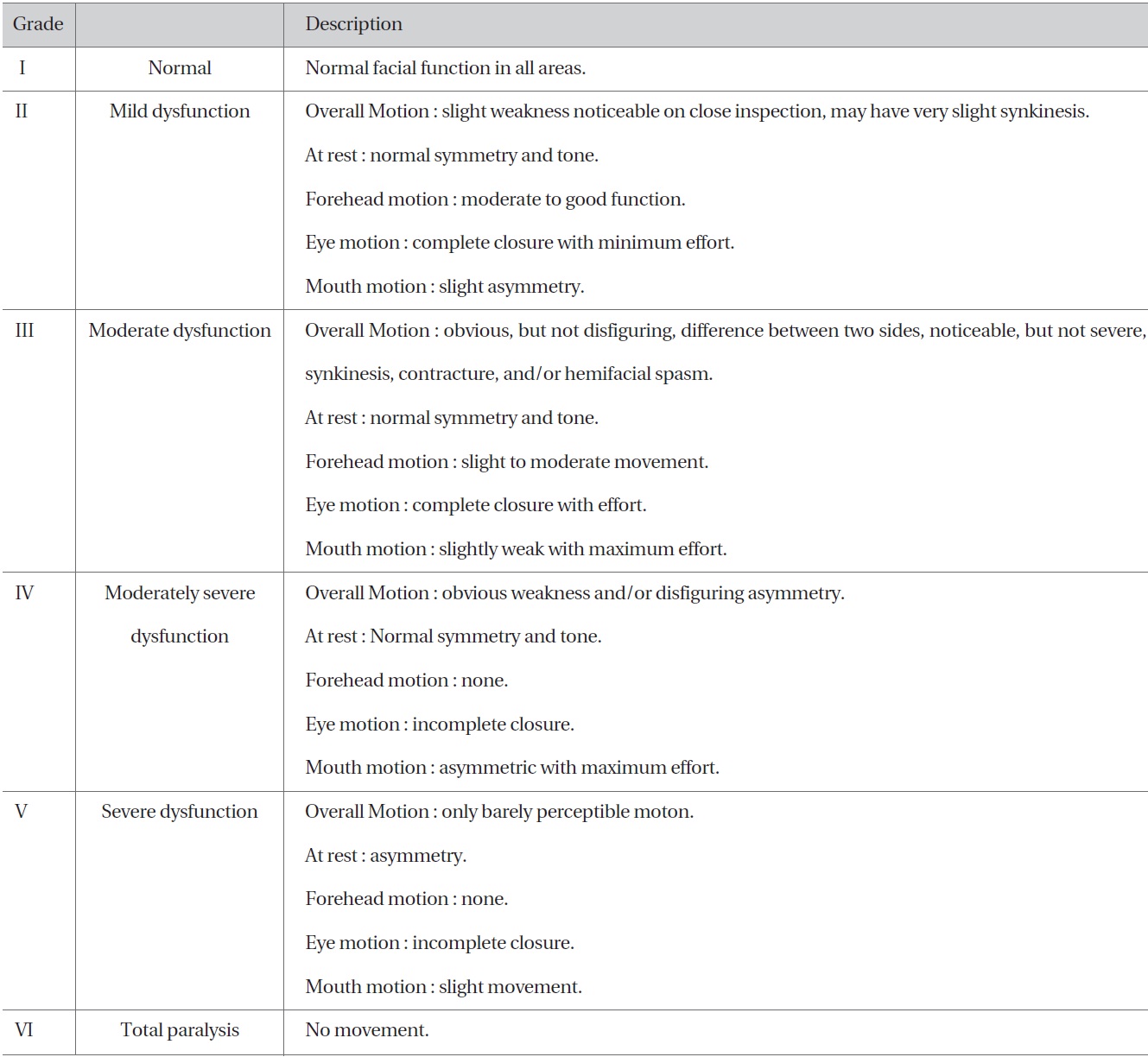
[Table 1] Gross grading system of House-Brackmann
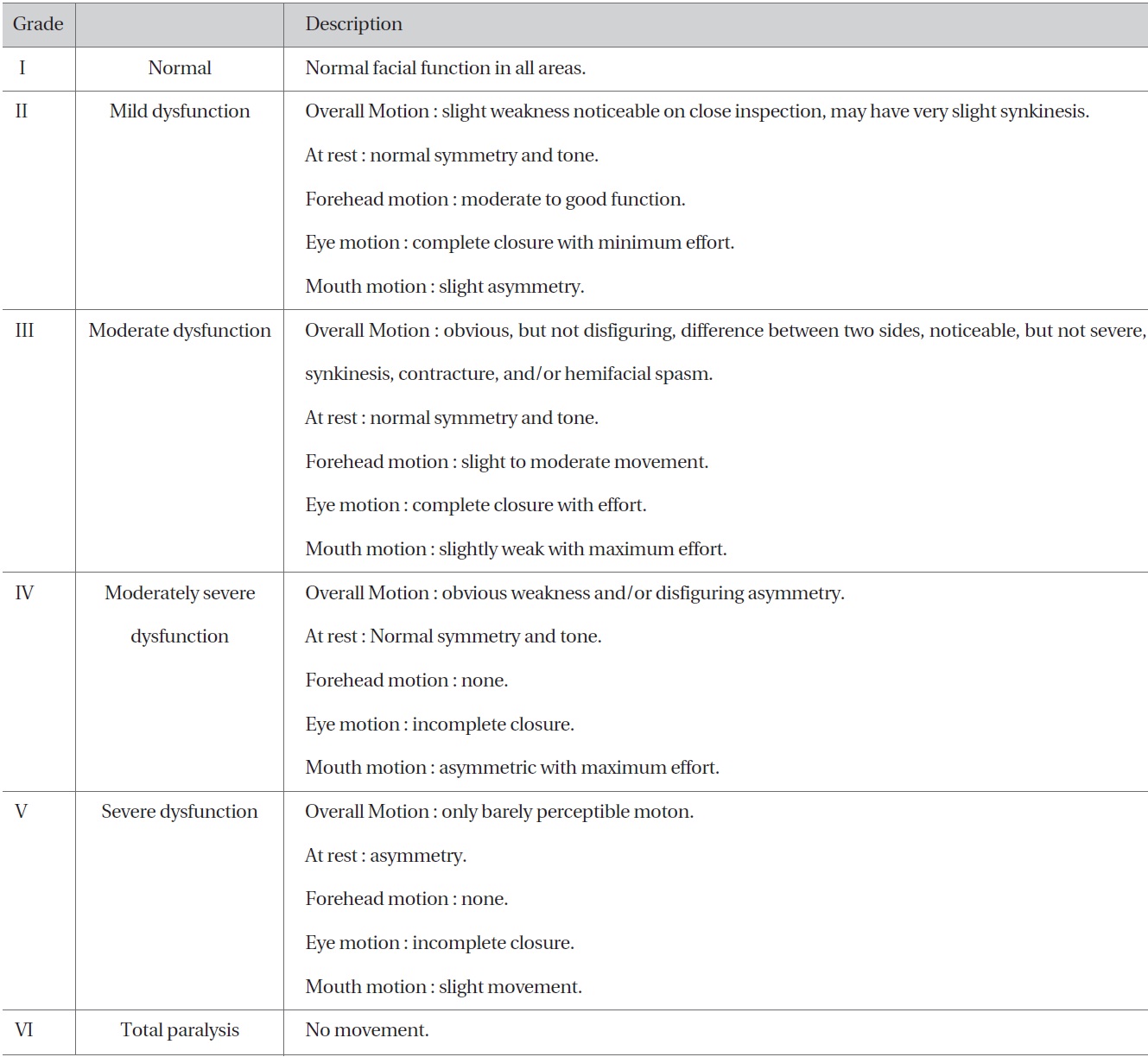
Gross grading system of House-Brackmann
on hominis placenta pharmacopuncture [10-12] and bee venom pharmacopuncture [13,14], but few clinical reports address the effects when rhizoma pharmacopuncture is within combination with other treatment modalities.
In this report, the authors present significant results obtained by analyzing the effectiveness and the safety of rhizoma pharmacopuncture as an accompanying method of treatment for patients with peripheral facial paralysis.
The subjects of this study were a total 70 patients who were inpatients at the Oriental Hospital of Daejeon University between January 1, 2011, and May 31, 2012, who showed no abnormal findings on pathological examinations, and were diagnosed by using physical examination as having peripheral facial paralysis. The patients were divided into those who were treated with or without pharmacopuncture. For a retrospective investigation, Specifically, The patients received three different interventions. Eleven (11) patients were treated with acupuncture and alcohol Dioscorea rhizoma pharmacopuncture (ADG), 25 patients with acupuncture and distillation Dioscorea rhizoma pharmacopuncture (DDG), and 34 patients with acupuncture and non-Dioscorea rhizoma pharmacopuncture (NDG). The resulting data were analyzed.
As for acupuncture, 0.20 × 30 ㎜ stainless-steel needles (Dongbang, Korea) were used. The patients underwent treatment twice per day in the hospital and two or three times per week as outpatients after discharge. The clinically-used meridians included jiache (ST6), dicang (ST4), chengchiang (CV24), yifeng (TE17), yingxiang (LI20), sibai (ST2), yangbei (GB14), hegu (LI14), sizhukong (TE23), and cuanzhu (BL2) on the affected side. For the pharmacopuncture, as seen in Ko et al. [15], DDG and ADG were manufactured in an aseptic room at the Korean Pharmacopuncture Institute. After application of acupuncture, 1.0 cc disposable insulin syringes (Shina Corporation, Korea) were used to inject 0.05 to 0.1 cc of the pharmacopuncture into meridians such as cuanzhu, jiache, dicang, sibai, ermen, and yifeng. The total injection was 1.0 cc three times per week, with at least five injections. The depth of the needles did not exceed 5 mm on the basis of pharmacopuncturology [16] and previous studies [17]. Generation & restriction and acupuncture techniques
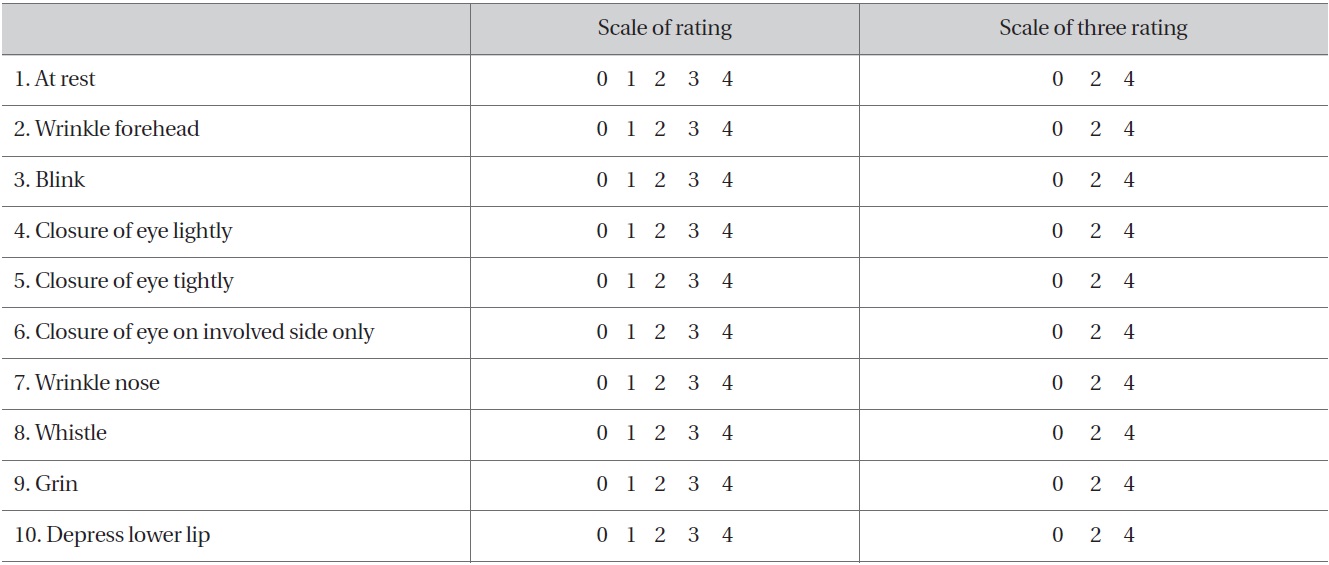
[Table 2] Yanagihara's unweighted grading system
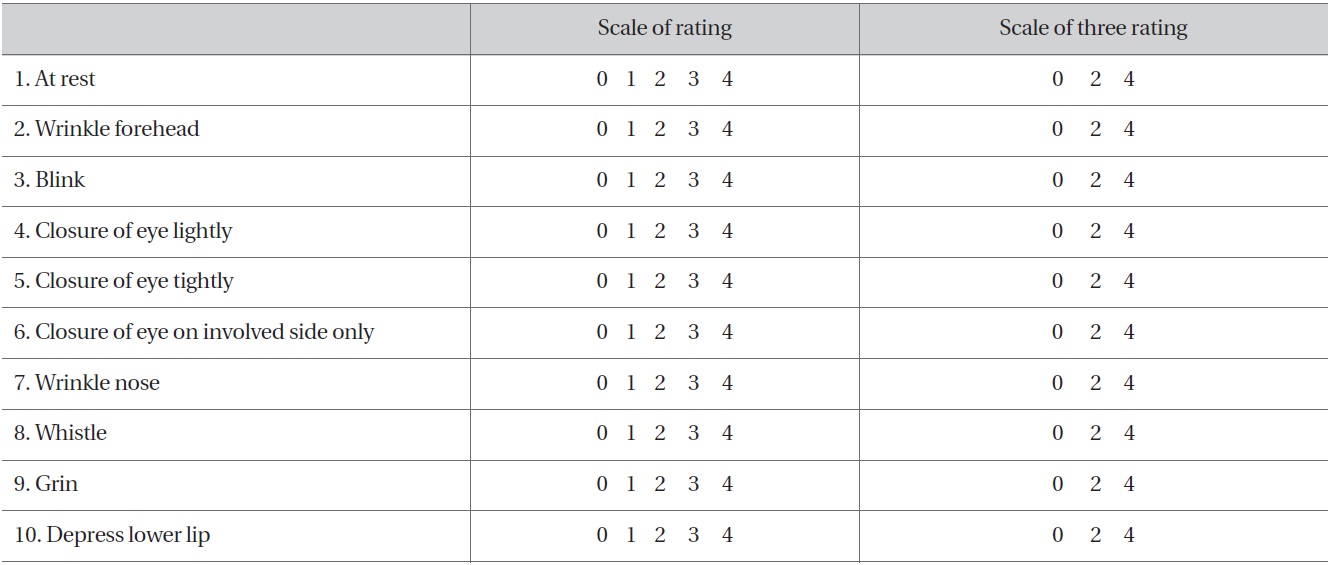
Yanagihara's unweighted grading system
were not used, and no retention time was applied because the needles were removed immediately after the drug had been injected.
For medicine administration, wasa A (Pueraria thunbergiana 8 g, Uncaria rhynchophylla 8 g, Bombysis Corpus 8 g, and Atractylodes japonica 6 g), wasa D (Astragalus membranaceus 8 g, Atractylodes japonica 8 g, Angelica gigas 8 g, and Rehmannia glutinosa 4 g) and pueraria ssangpai-tang (Paeonia japonica 10 g, Rehmannia glutinosa 4 g, Astragalus membranaceus 4 g, and Angelica gigas 4 g) were applied on the basis of changes in the patients' findings. Steroids were orally administered to relieve initial inflammation, after a heal the dosage was gradually reduced. Artificial tears and oculentum were applied according to the symptoms.
The House-Brackmann grading system (H-B grade) [18] for integrally assessing facial paralysis and secondary concomitant symptoms at the same time were used to measure the degree of facial paralysis for each group. The H-B grades were obtained before treatment to determine the facial paralysis baseline. They were obtained again after one week of treatment and after two weeks of treatment for the purposes of comparison, a comparative analysis of the H-B grades was performed based on the descriptions in table 1. Using Yanagihara's unweighed grading system [19], we conducted a total of four assessments: baseline and after five days, ten days, and 15 days of treatment. Yanagihara's score (Y-Score) uses a 5-point system: 4-normal, 3-slight, 2-moderate, 1-severe, and 0-total. All the Y-scores were added to obtain the final scores for assessment, and the maximum score was 40 points (Table 2).
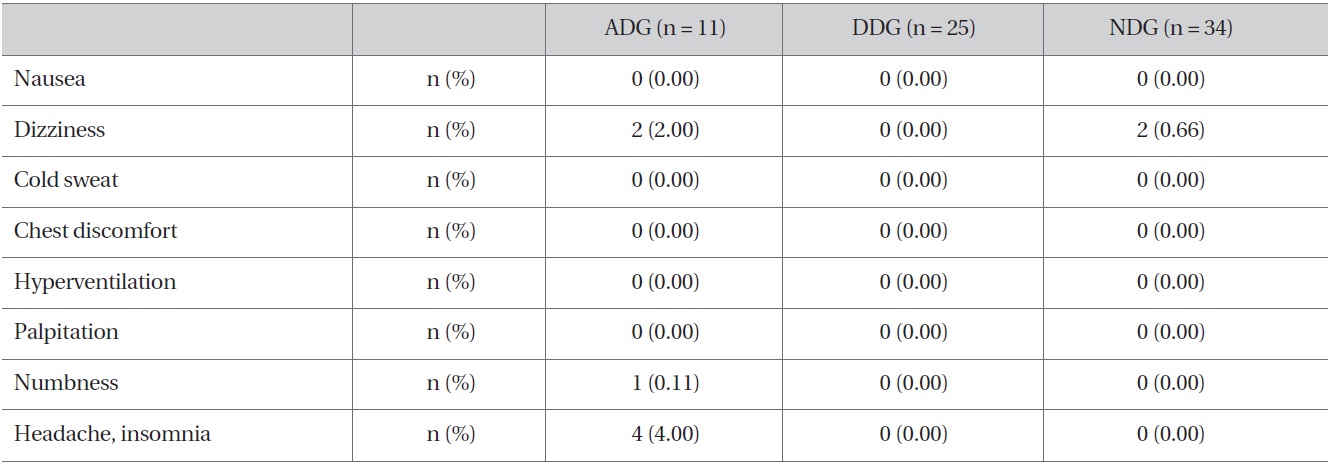
The physical responses to be examined included skin flares, itching sensation, burning sensation, edema, subcutaneous bleeding, abscess caused by infection, and induration. Their responses were investigated using the method of Ko et al. [15]. As for subjective symptoms, nausea, dizziness, cold sweat, chest discomfort, hyperventilation, palpitation, numbness, headache, and insomnia were investigated using the method of Ko et al. [15].
For the demographic data and the clinical histories at initial treatment for the groups, continuous data are presented as means, standard deviations, minimum values, and maximum values while categorical data are presented as frequency tables. For a comparative analysis of the demographic and the basic data for each group, the Kruskal-Wallis one-way ANOVA was applied to continuous variables while Pearson's chi-square test or Fisher's exact test was applied to categorical variables. When variables showed statistically significant differences between the groups, a generalized linear mixed model was used to correct the differences in the effectiveness assessment and the safety assessment for the statistical analysis. All the statistical analyses were conducted with the Windows'SAS Release 8.02, and a 5% significance level was considered statistically significant.
3.1. General characteristics of the subjects
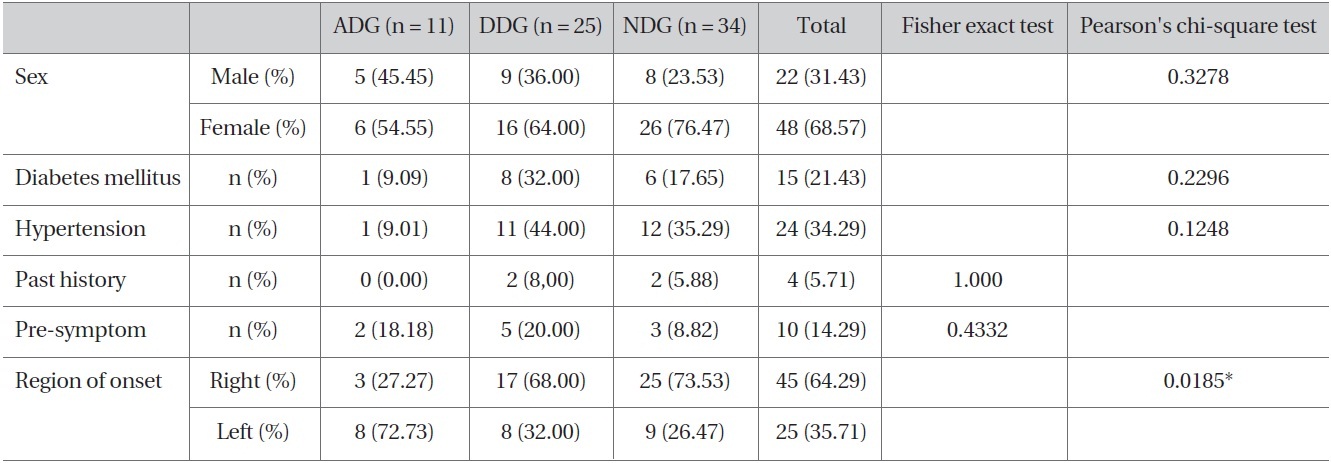
The demographic investigation showed no differences in clinical characteristics were found among the three groups, but region of onset showed statistical significant
[Table 3] Clinical characteristic of three groups with ADG, DDG, NDG.
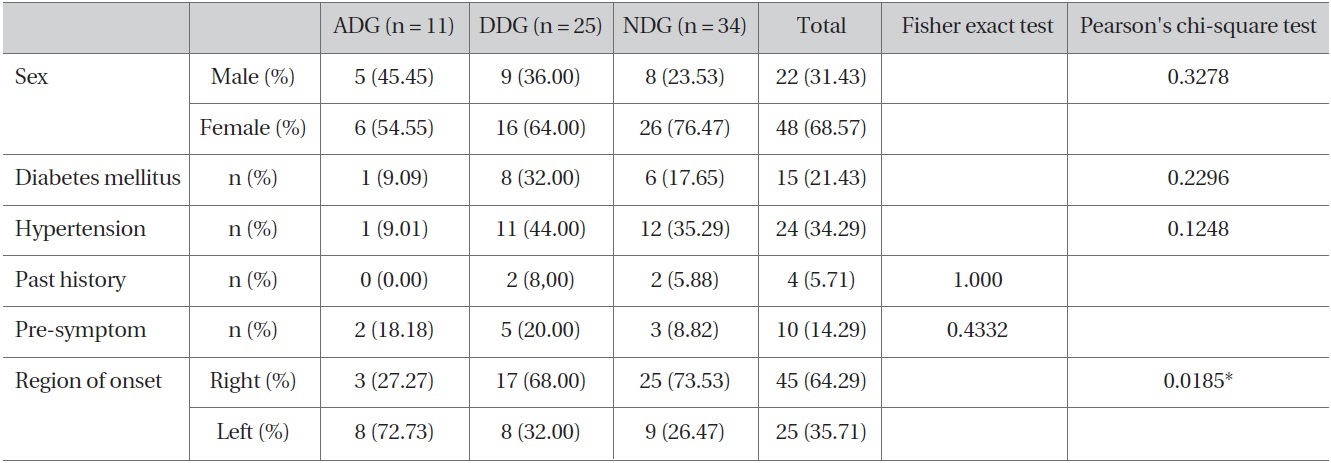
Clinical characteristic of three groups with ADG, DDG, NDG.
difference between the treatment groups (
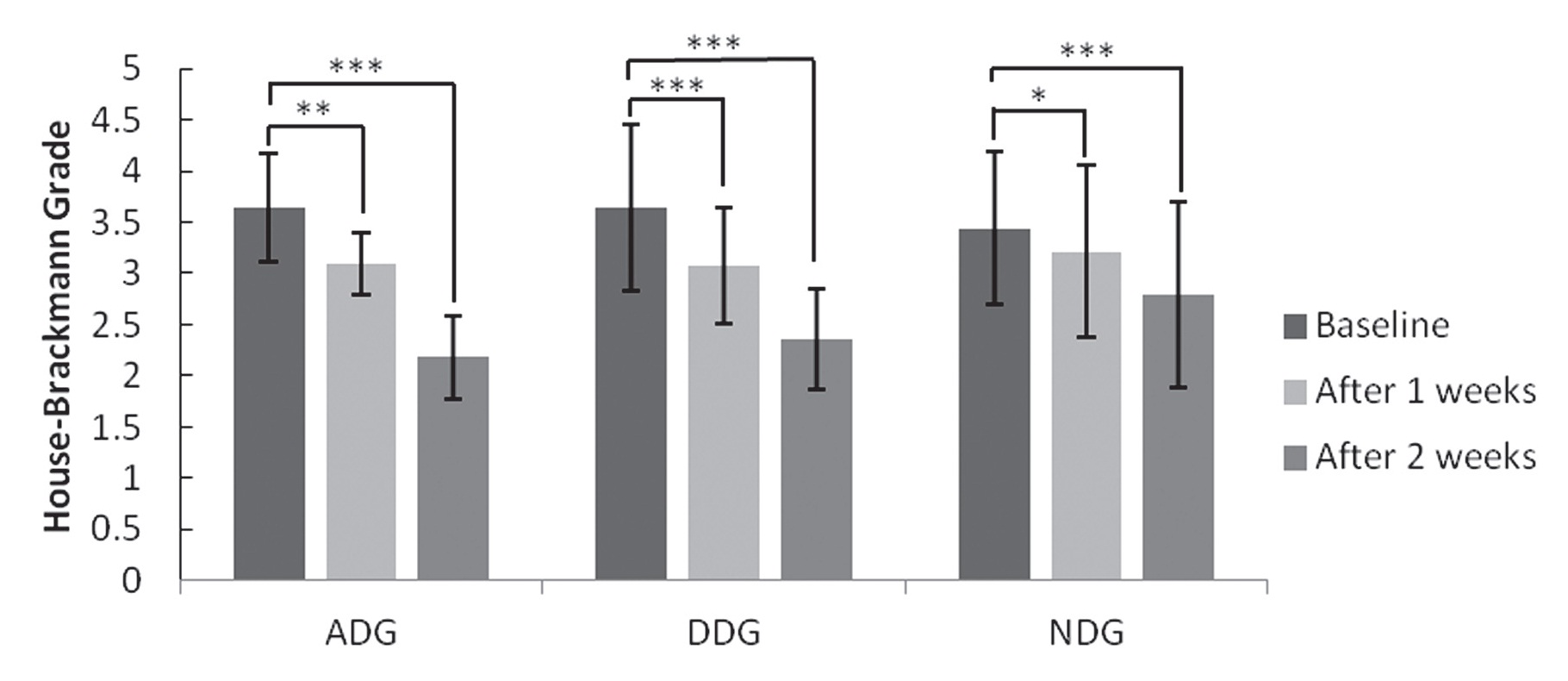
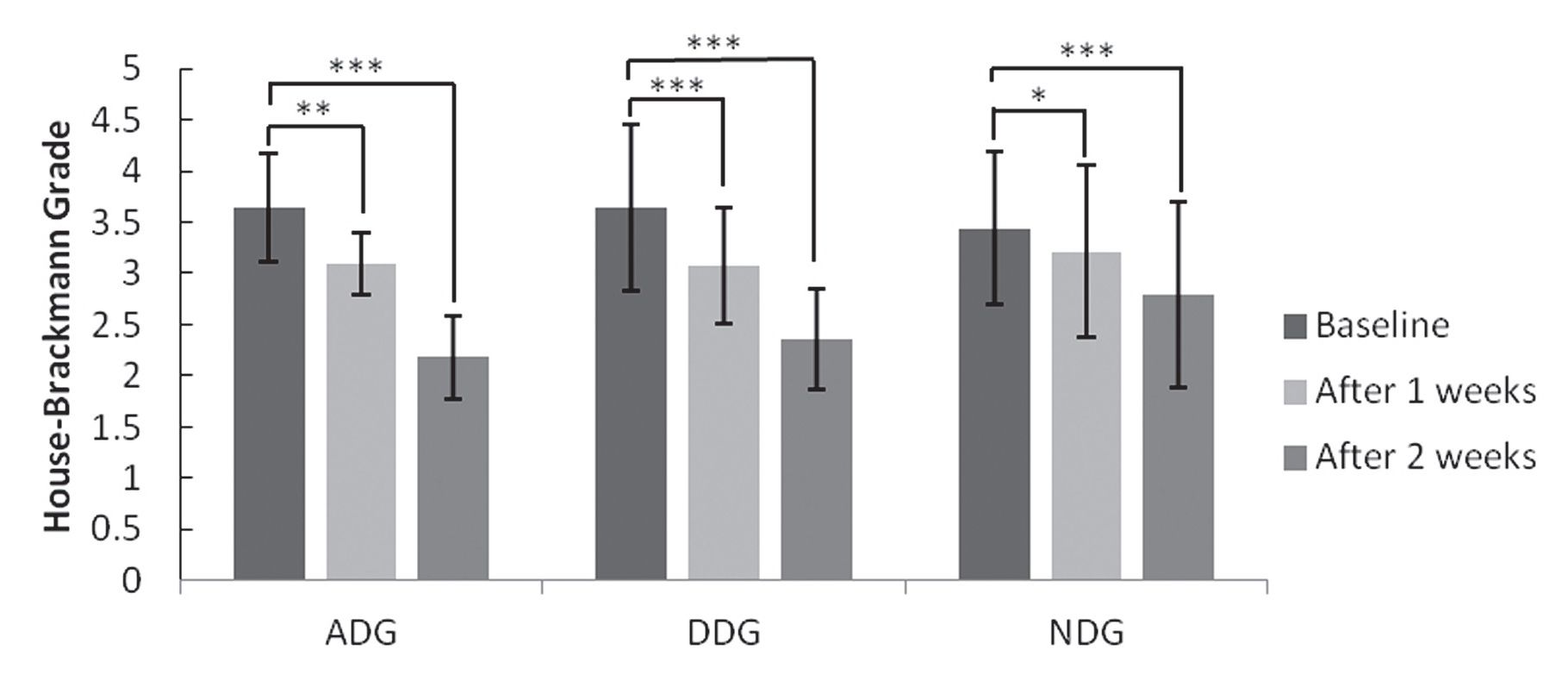
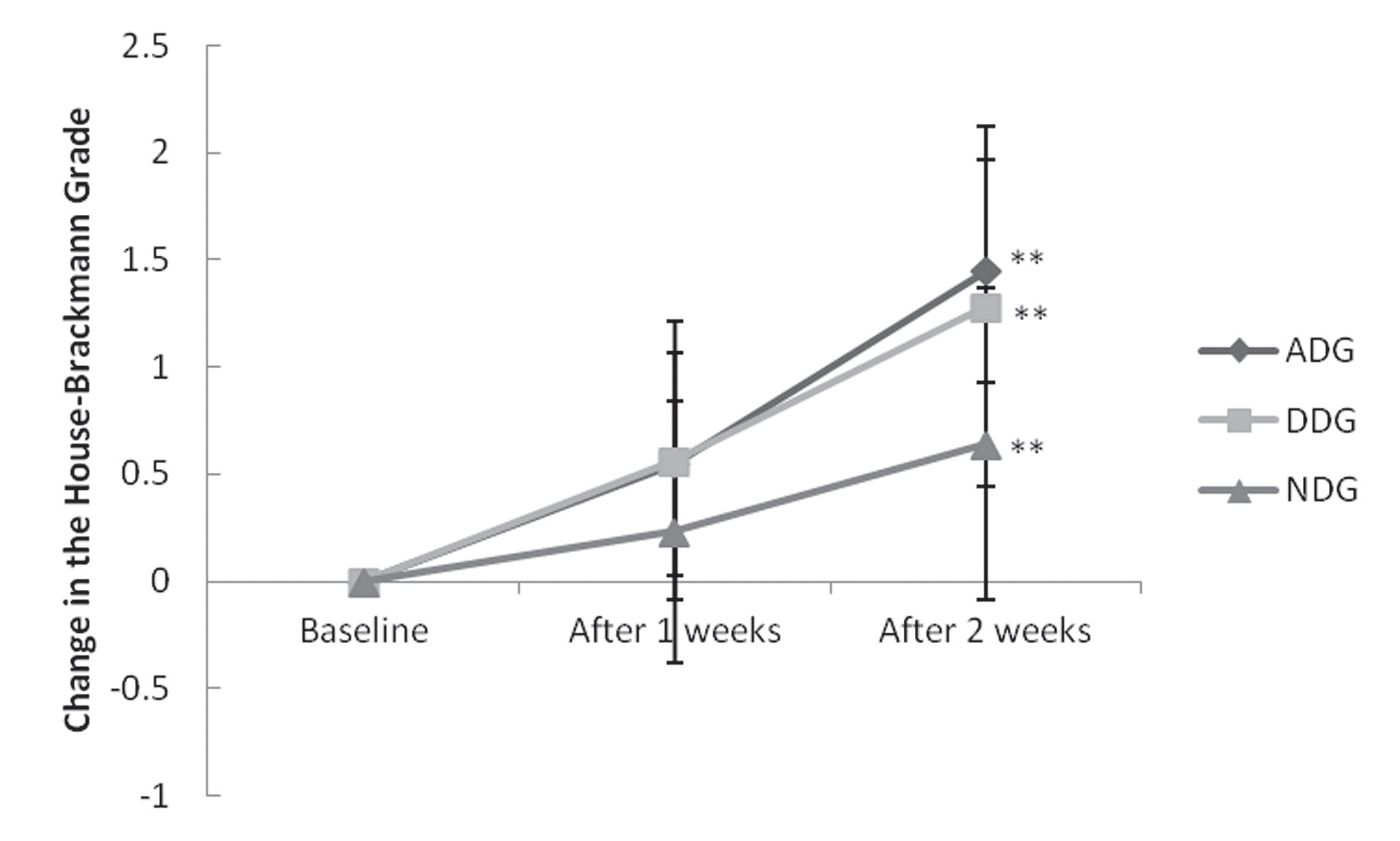
The H-B grades of the patients of all treatment groups at the baseline showed no statistically significant difference (Fig 1).
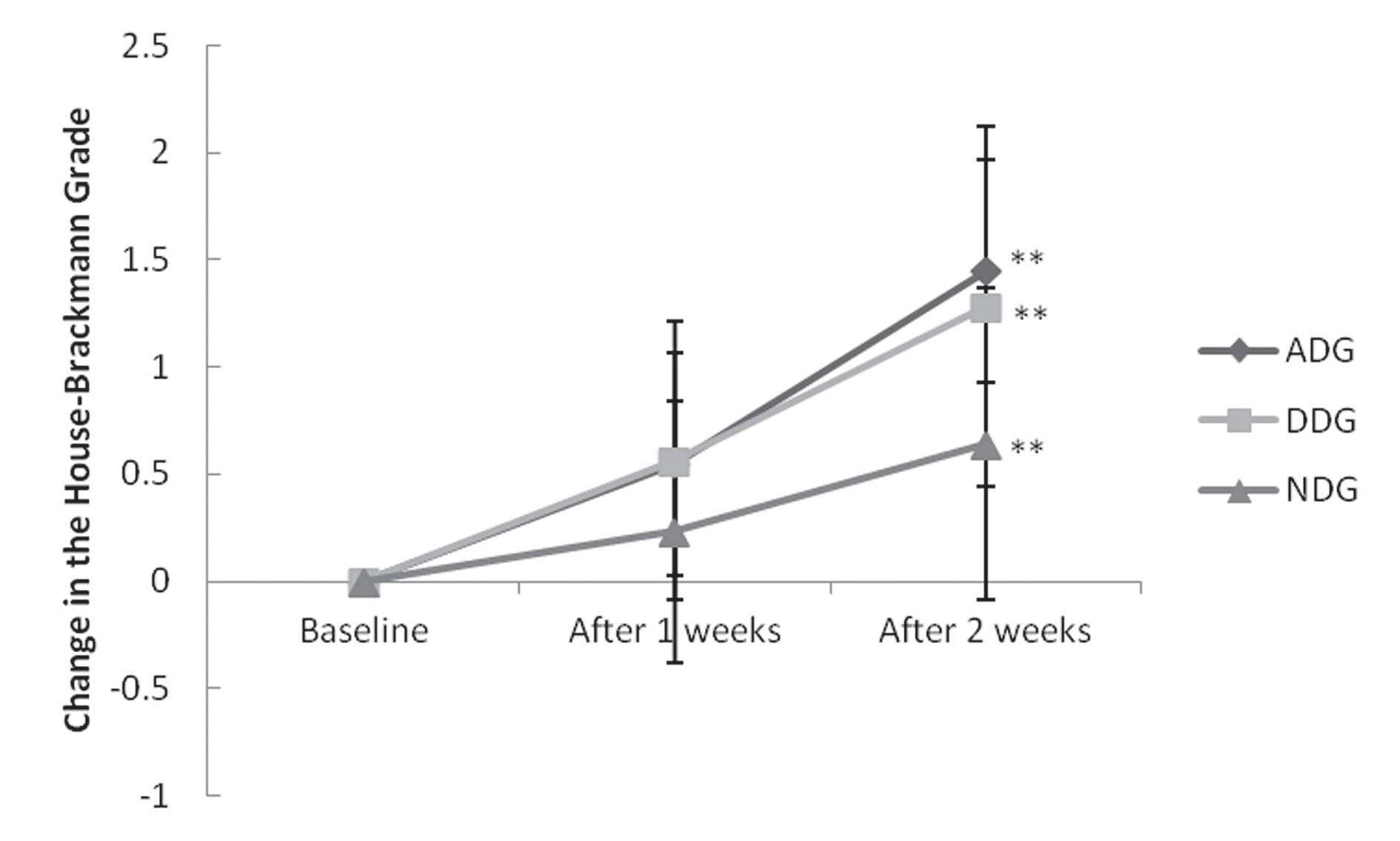
The H-B grade changes after one and two weeks of treatment, when compared to the grades at the baseline in each group, showed statistically significant change in all groups (Fig 1). Verification of the significant differences in the changed H-B grades between the three groups after one week of treatment at alert levels showed statistically significant difference in the treatment effects between the groups (
Based on the above results, a Tukey honestly significant difference was conducted to identify which groups showed significant mean differences. Significant differences were noted the ADG and the NDG groups and between the DDG and the NDG groups after two weeks of treatment (
At the baseline, no statistically significant differences were
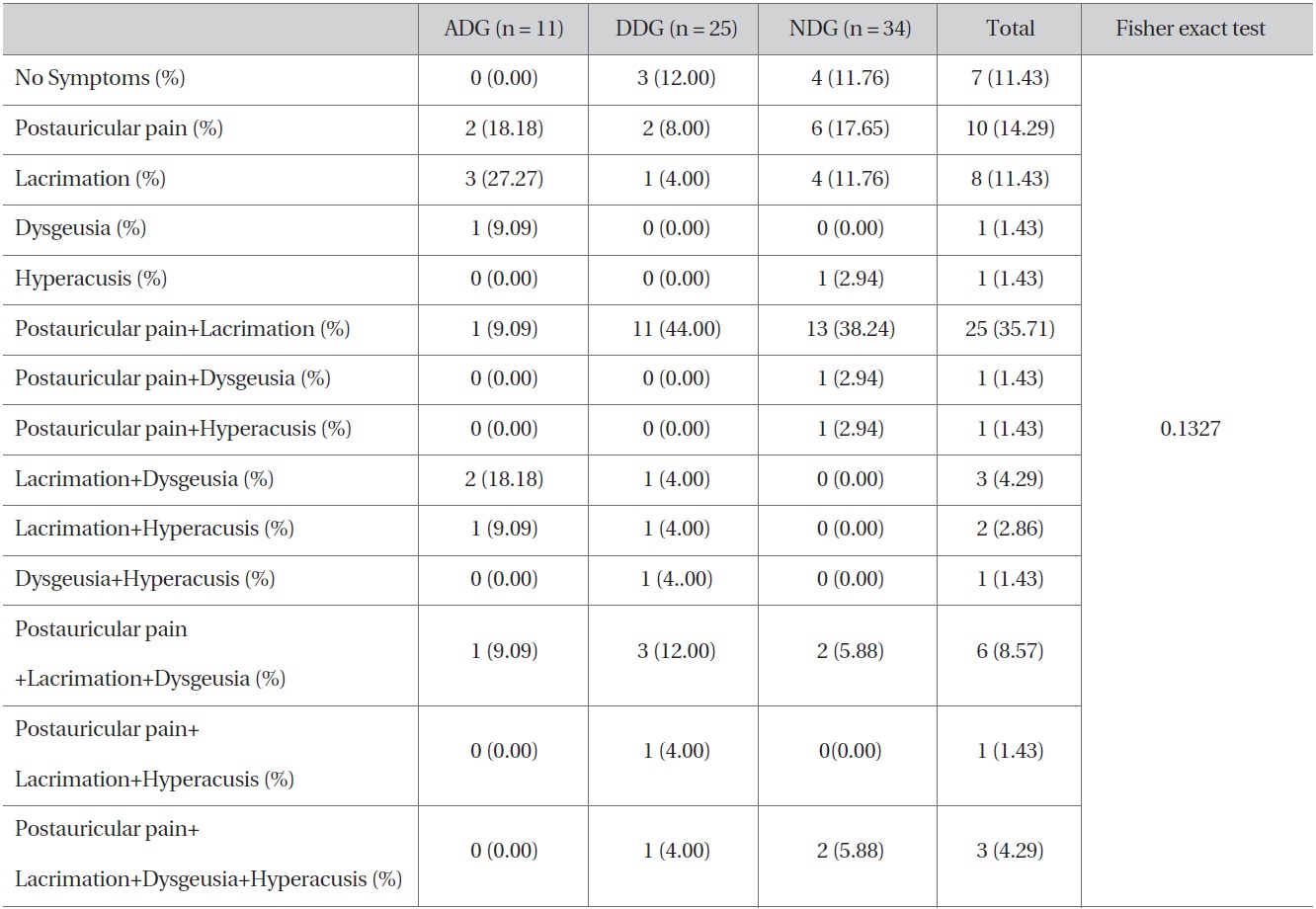
[Table 4] Distribution of patients with co-symptoms at on the onset
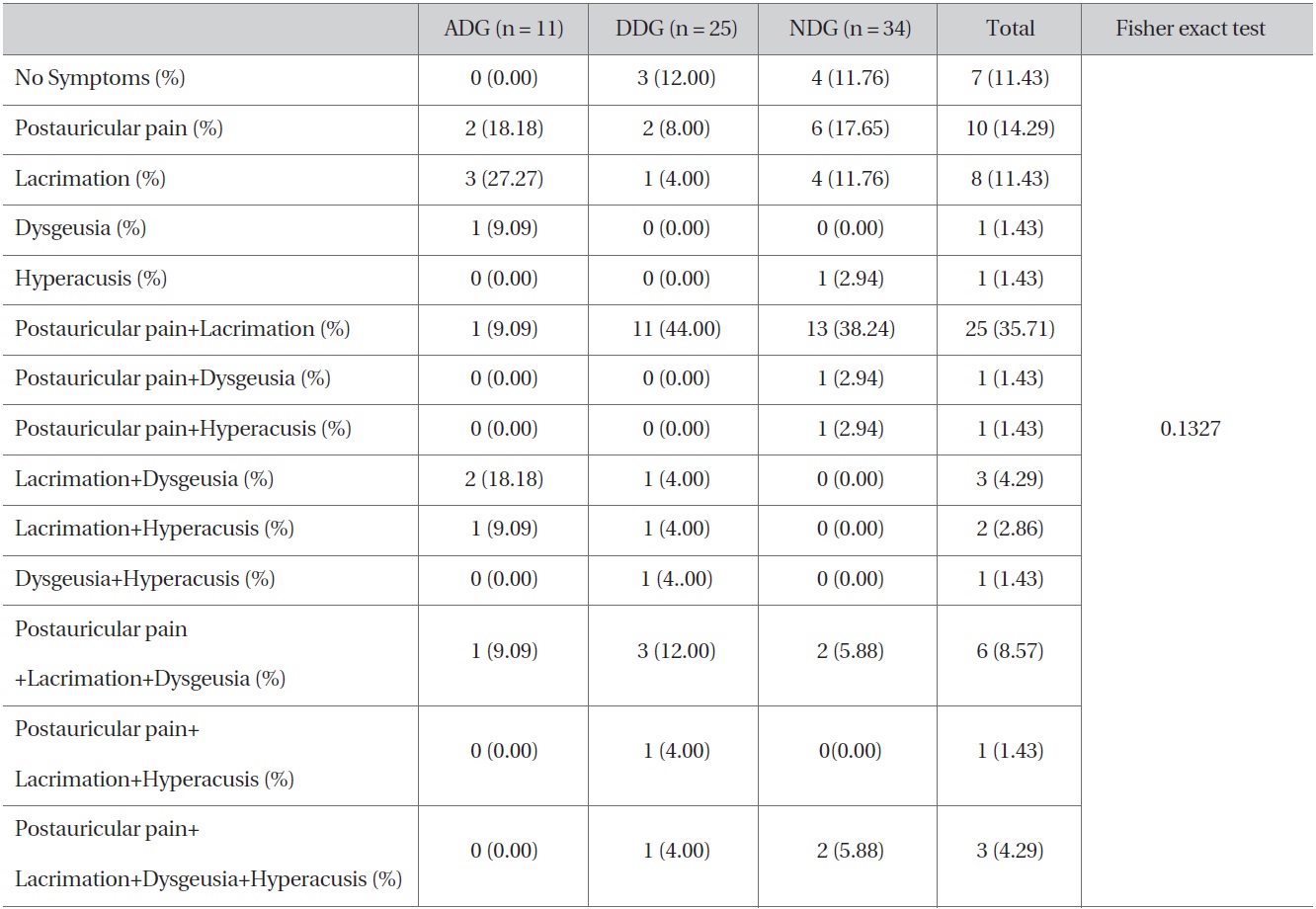
Distribution of patients with co-symptoms at on the onset
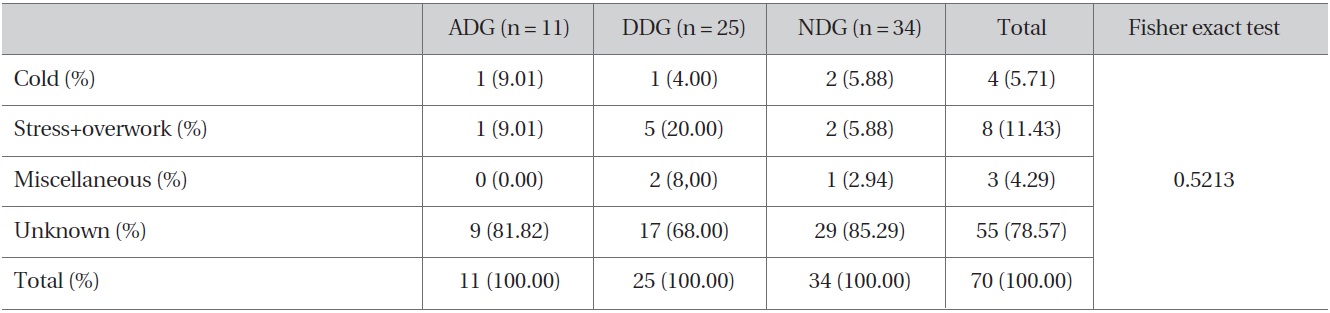
[Table 5] Distribution of disease factors
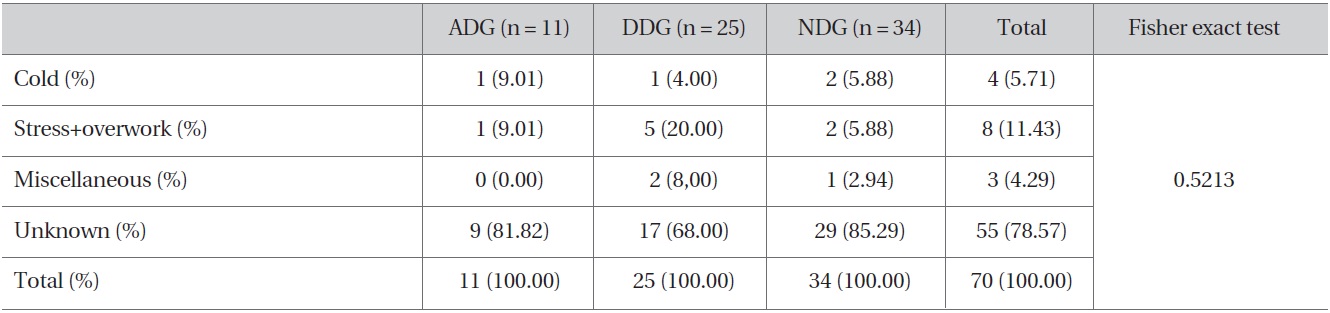
Distribution of disease factors
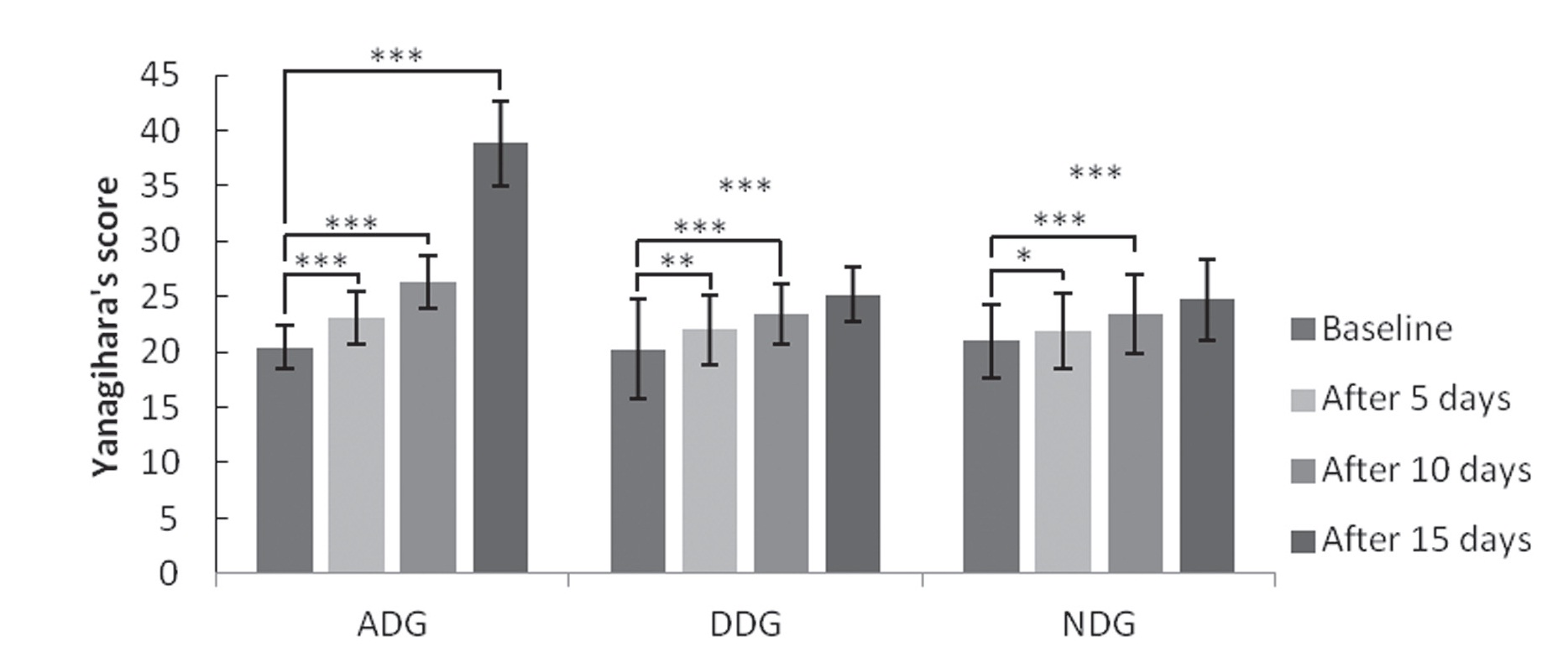
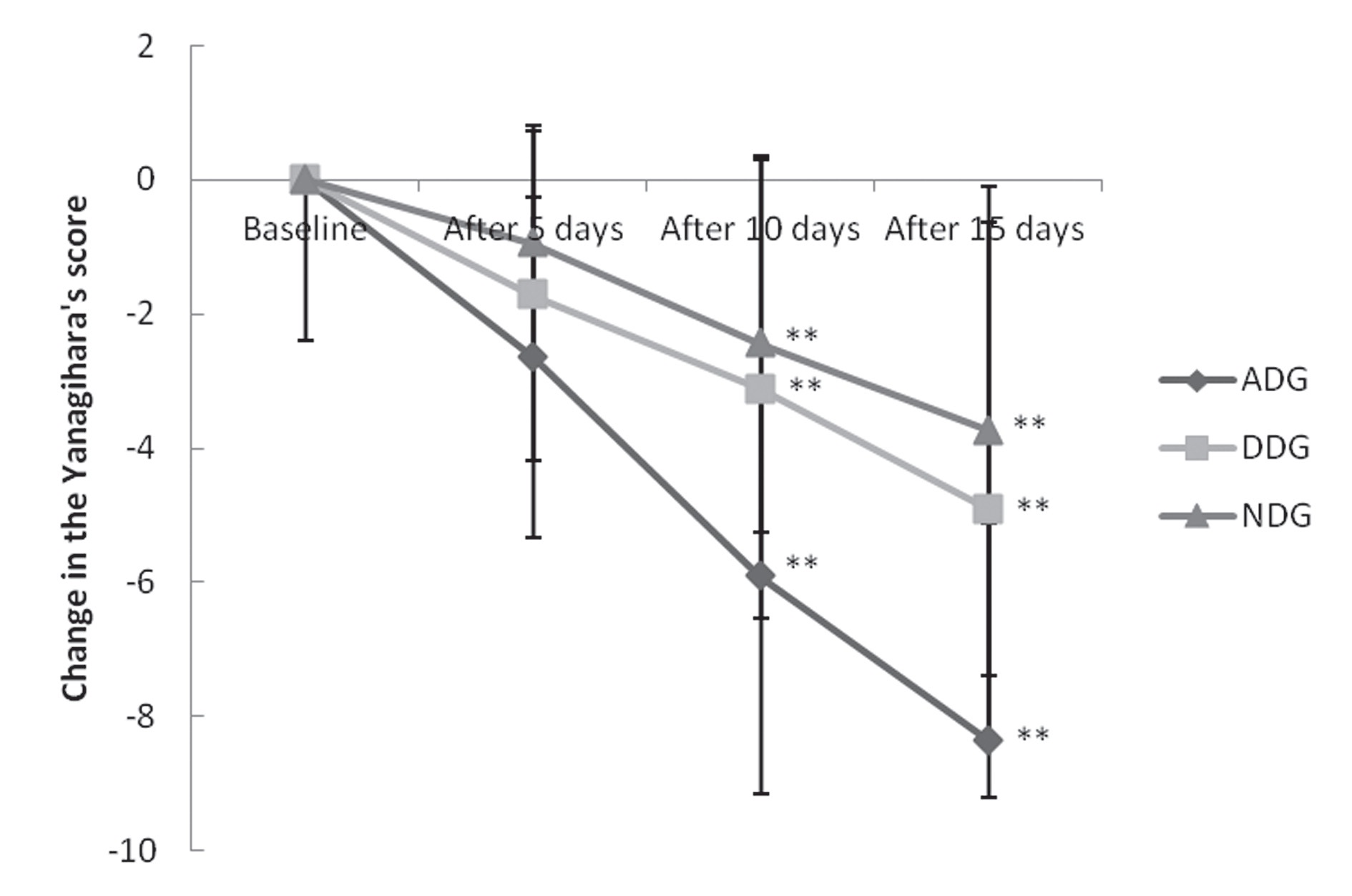
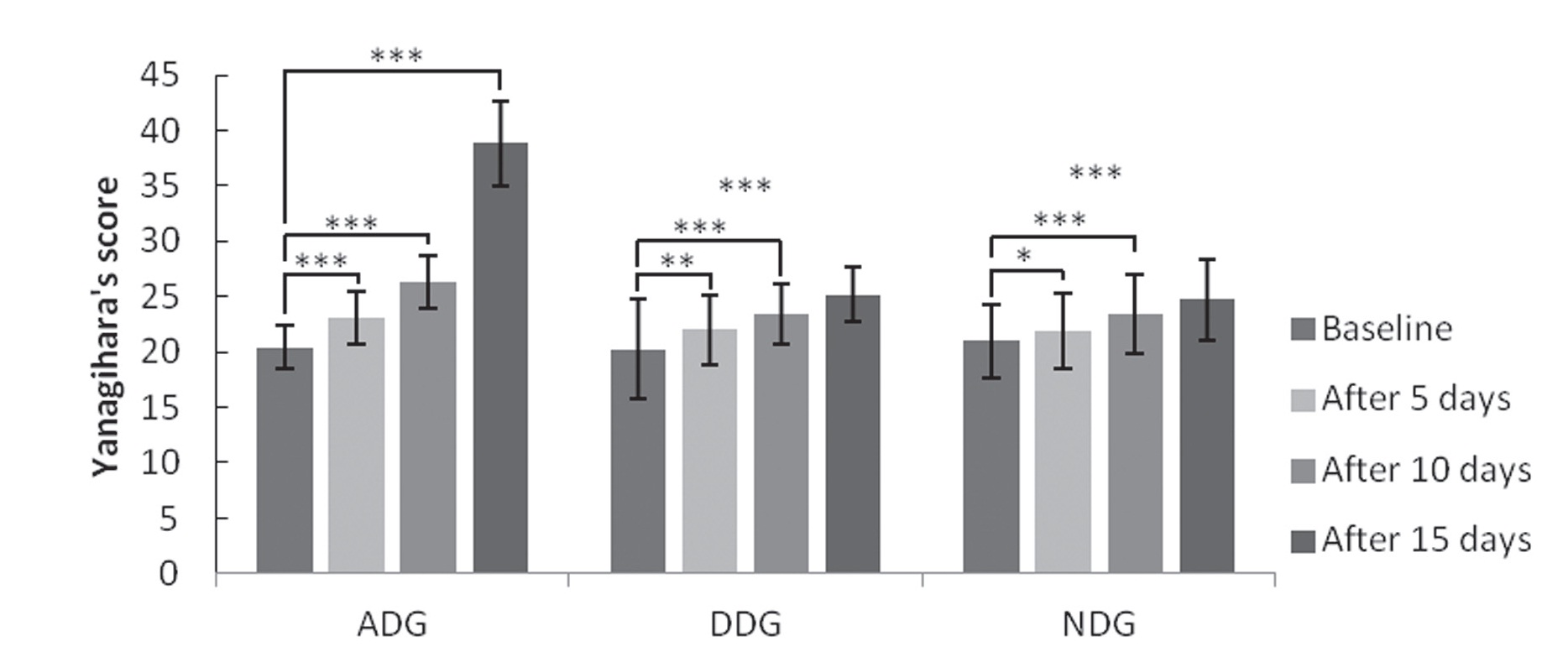
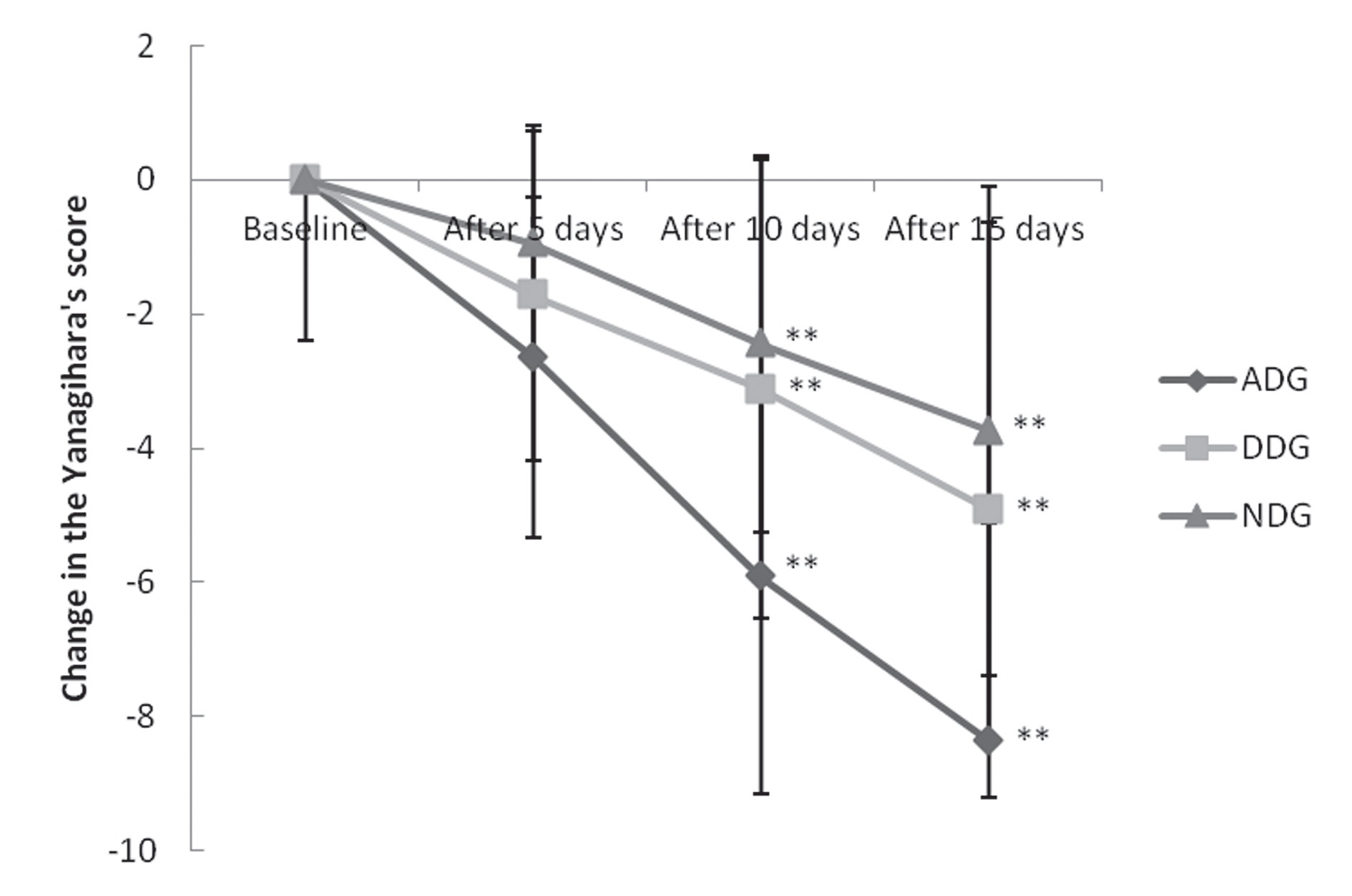
found in the Y-scores of the groups (Fig 3).
Verification of the significant differences in the Y-score changes after 5, 10, and 15 days of treatment in each group indicated that all the groups showed significant Y-score changes based on the treatment period (Fig 3). Verification of the significant differences in changed Y-scores between the three groups after 5, 10, and 15 days of treatment showed statistically significant differences in the treatment
effects between the ADG, the DDG, and the NDG groups after 5 days at alert levels (
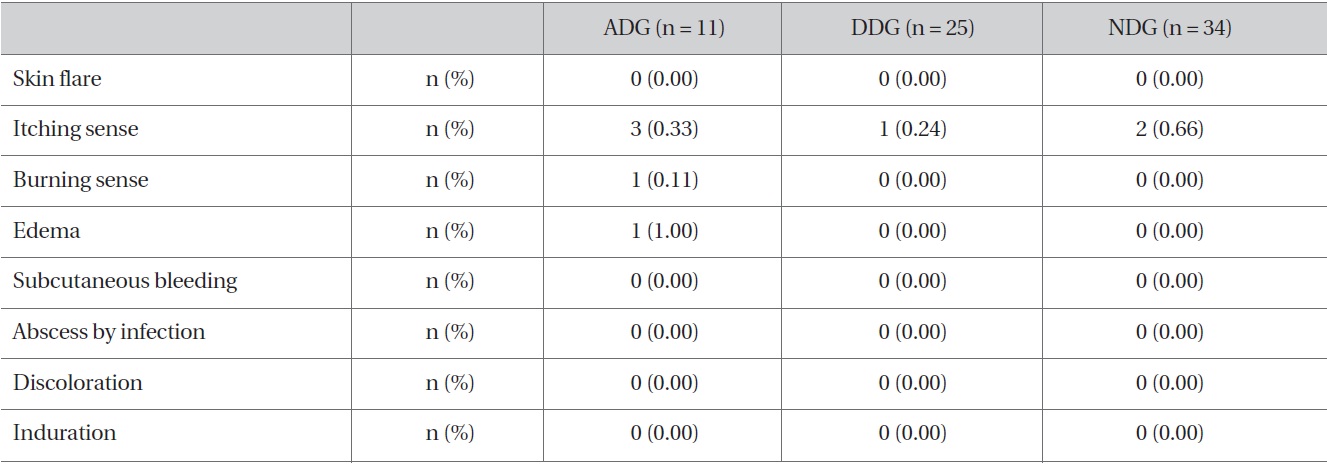
[Table 6] Physical responses after injections for three groups, ADG, DDG, and NDG.
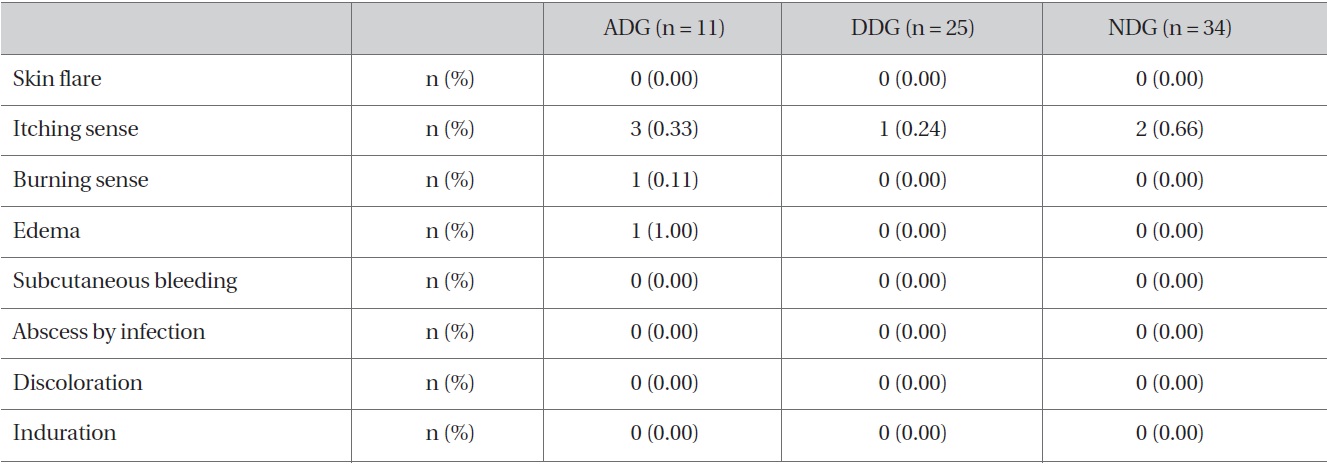
Physical responses after injections for three groups, ADG, DDG, and NDG.
3.3. Results of safety assessment
On the safety assessment, ADG group showed pain, skin flare, and edema, the DDG group showed pain, and the NDG group showed pain (Table 6). As to subjective symptoms, the ADG group showed 4 cases of nausea and dizziness and 1 of numbness, and the NDG group showed 2 cases of dizziness (Table 7).
In Oriental medicine, peripheral facial paralysis is included in Guangeosa (Bell's palsy), and various discussions have been conducted on the etiology and the treatments of the disease. Recently, application of acupuncture accompanied by various pharmacopuncures has been variously used, and hominis placenta pharmacopuncture [10-12] and bee venom pharmacopuncture [13,14] have mostly been used as the accompanying pharmacopuncture. However, few clinical reports address the efficiency of accompanying Dioscorea rhizoma pharmacopuncture.
Recent studies of Dioscorea rhizoma pharmacopuncture
[Table 7] Subjective symptoms after injections for three groups, ADG, DDG, NDG
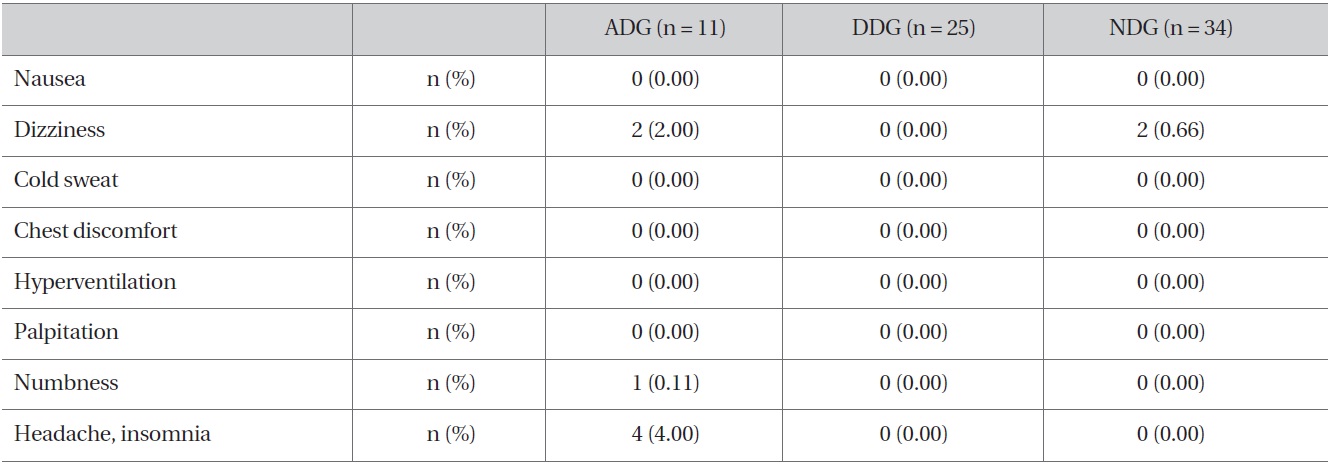
Subjective symptoms after injections for three groups, ADG, DDG, NDG
by Lee et al. [20] reported that Dioscorea rhizoma injected into the injured sciatic nerve of a mouse improved regeneration in the acral axon in the sciatic nerve and enhanced production of various proteins related to axon regeneration. Such nerve regeneration by Dioscorea rhizoma pharmacopuncture is significant in that the pharmacopuncture may be used for illnesses in the nervous system, such as Bell's palsy.
In this context, the authors of this study selected patients diagnosed by physical examination as having peripheral facial paralysis after admission to the Daejeon Oriental Hospital of Daejeon University between January 1, 2011, and May 31, 2012, 11 cases treated with acupuncture and alcohol Dioscorea rhizoma Pharmacopuncture (ADG), 25 cases treated with acupuncture and distillation Dioscorea rhizoma Pharmacopuncture (DDG), and 34 cases treated with acupuncture and non-Dioscorea rhizoma Pharmacopuncture (NDG), for clinical comparisons in order to analyze, based on the results of the previous studies, the efficiency and the safety of Dioscorea rhizoma pharmacopuncture for patients with peripheral facial paralysis. The Clinical characteristics on initial examination showed no statistically significant differences between the three groups (ADG, DDG, and NDG) (Table 3).
As for the co-symptoms at the onset, many involved two symptoms rather than only one symptom. The fact that postauricular pain was the most frequent co-symptoms at the onset was consistent with the results of Kim et al. [13] and Yang and Song. [14]. The co-symptoms at the onset did not show statistically significant differences between the groups (Table 4). The disease factor was unknown for 55 of the 70 cases (Table 5), which were consistent with the results of Kim et al. [13] Also, the disease factors showed no statistically significant differences between the groups (Table 5).
The authors measured and compared the degrees of peripheral facial paralysis by using the House-Brackmann grading system and Yanagihara's unweighed grading system. As for the H-B grades at baseline, the means and standard deviations of the three groups indicated the H-B grades for the NDG group were slightly lower, but the difference was not statistically significant. As for the Y-scores at baseline, the means and the standard deviation of the three group indicated that those of the NDG group were slightly higher, but without statistical significance. Consequently, the degrees of peripheral facial paralysis were similar between the three groups.
When changes by treatment period were compared for the ADG, the DDG, and the NDG groups, the H-B grades showed significant increases from the baseline after one and two weeks of treatment (
As for the changes by treatment periods of the three groups, the H-B grades showed statistical significance at alert levels between the groups after one week of treatment (
The changed Y-scores among the three groups by treatment periods showed that the treatment effects for the ADG, the DDG, and the NDG groups were statistically significant at alert levels after 5 days of treatment (
The Y-Scores after 10 and 15 days of treatment were higher in the ADG groups than in the DDG and the NDG groups, indicating that the results were consistent with the analysis via the H-B grades and that the alcohol Dioscorea rhizoma pharmacopuncture may be the most effective.
As for the physical responses during the treatment with accompanying Dioscorea rhizoma pharmacopuncture, the ADG group showed pain, burning sensation, and edema, the DDG group showed no specific responses, and the NDG group showed only pain (Table 6). As for the subjective symptoms felt by patients, the ADG groups had nausea and dizziness, and the NDG group had dizziness (Table 7). However, Dioscorea rhizoma pharmacopuncture may be safe for the human body because in most of the above cases, the only abnormal finding was pain, with no other severe physical responses or subjective symptoms.
In conclusion, acupuncture treatment was, accompanied by Dioscorea rhizoma pharmacopuncture in order to enhance the effects of treatment for peripheral facial paralysis the combined therapy led to improvements as the treatment continued. Significant differences in treatment results were noted for different treatment times, with longer treatment times producing better results.
The authors of this study conducted a retrospective investigation for a total 70 cases of patients, who were inpatients at Oriental Hospital of Daejeon University between January 1, 2011, and May 31, 2012, and who were diagnosed as having peripheral facial paralysis by physical examination. For comparative analysis, the patients were divided into 11 patients who were treated with acupuncture and ADG, 25 patients who were treated with acupuncture and DDG, and 34 patients who were treated with acupuncture and NDG. The results were as follows:
1. The changed H-B grades indicated significant improvements in all the three groups, and the ADG and the DDG groups showed significant results after two weeks of treatment when compared to the NDG group.
2. The changed Y-scores indicated significant improvements in all three groups, and the ADG group showed significant results after 10 and 15 days of treatment when compared to the NDG group.
3. Dioscorea rhizoma pharmacopuncture may be safe for the human body because in most cases, the only abnormal finding was the pain caused by the application of pharmacopuncture.