Lumbago has been a distressing problem among human beings since they, unlike other animals, started to stand erect with both feet, and over 80% of the general population is reported to experience lumbago [1]. Lumbago and skelalgia are radiating pains to the lower back and legs. These terms just represent clinical symptoms, not disease entities or syndromes [2]. In Western medicine, the causes of lower back pain (LBP) are classified as discogenic, vertebral and abdominal. The main diseases causing lumbago are lumbosacral sprain, herniation of the intervertebral discs, spinal stenosis, spondylolysis, spondylolisthesis, spondylosis and osteoporosis [3]. The traditional Korean medical treatment of lumbago is mainly conservative, and the literature has reported various treatment options, including herbal medicine, acupuncture, physical therapy, chuna manual medicine, electro-acupuncture treatment and exercise. Many pharmacopuncture therapies, such as body acupuncture, Sa-am acupuncture, Dong-Si acupuncture, eight-constitution acupuncture, auricular acupuncture, hand-finger acupuncture and pharmacopuncture, are used in various combinations [4].
Pharmacopuncture therapy selects highly effective herbs for treating human disease. Effective pharmacopuncture fluid is extracted from herbs and is injected into the meridian points or sore spots. It is a mixed treatment option that combines the meridian system and medical action [5]. Many researchers currently use pharmacopuncture therapy for the treatment of lumbago and skelalgia. Cha et al. [6], Yu et al. [7], and Lee et al. [8] performed a combination of acupuncture therapy and bee venom pharmacopuncture on patients with herniation of the lumbar intervertebral discs. This combined treatment suggests that bee venom pharmacopuncture may have an effect on the disease. Yoon et al. [9] confirmed the effects of Carthalni Flos pharmacopuncture (Saflower pharmacopuncture) in lumbago patients. Lee et al. [10] showed that bee venom pharmacopuncture and Jungsongouhyul pharmacopuncture, either alone or in combination, had an impact on patients with lumbago or skelalgia. Despite several investigations regarding the effects of pharmacopuncture on patients with lumbago and skelalgia, whether its curative effects are attributed to the pharmacopuncture itself, psychological effects or a natural course is controversial. Based on the results of Seo and Xue [11], we conducted a comparative study of patients with lumbago and skelalgia who had been treated with Chukyu (spine-healing) pharmacopuncture or with saline (Normal Saline; NS) pharmacopuncture.
The research involved patients who visited the acupuncture & moxibustion department at Dong-Eui University Hospital of Oriental Medicine for lumbago from July 5, 2011, to January 31, 2012. Via randomization, a total of 45 subjects who had lumbago and skelalgia were divided into two groups: the Chukyu (spine-healing) pharmacopuncture-treated group (experimental group) and the normal saline (NS) pharmacopuncture-treated group (control group). Selection criteria were as follows:age over 50, but less than 90; unilateral or bilateral lumbago, radiating pain, or pain as the chief complaint; visual analog scale (VAS) value over 5 on the pre-test; and lumbago for longer than a month. Exclusion criteria included the following:lumbosacral history of trauma or bone fracture; hypersensitivity or active skin disease; active infectious disease requiring medical care for the entire body; and mental diseases, alcoholism and/or drug addiciton.
We used Chukyu (spine-healing) pharmacopuncture from the Korean Pharmacopuncture Institute for the experiment group. The constituents of Chukyu (spine-healing) pharmacopuncture are Cervi Parvum Cornu (deer antlers), Moschus (musk), Angelicae Gigantis Radix, Cnidii Rhizoma, Ostericii Radix, Angelicae Pubescentis Radix, Astragali Radix, and Scolopendra, which are extracted via low-temperature low-pressure extraction in an aseptic room at the Korean Pharmacopuncture Institute. The control group was injected with 20 cc of normal saline (NS) pharmacopuncture consisting of isotonic sodium chloride from Choongwae Pharma Corporation.
With PHYTOject disposable 2cc syringes (SIR Medical Co, Ltd.) and 30G needles (1 and

inch, Jungrim Medical Device Company), the subjects were injected 0.1~0.3cc and 2~3cm deep, respectively, for each meridian point once a day, twice a week, for a total of eight injection per month. The procedures were mainly performed at the Samchosu (BL22), Sinsu (BL23), Gihaesu (BL24), Daejangsu (BL25), and Ashi points. The acupuncture needles were disposable stainless-steel filiform needles (0.20 mm x 30 mm) from Dongbang Acupuncture, Inc. Following the meridian points, the needles were inserted 5~10 mm deep once a day, twice a week, for a total of eight per month. The treatment was at the Samchosu (BL22), Sinsu (BL23), Gihaesu (BL24), Daejangsu (BL25), Jisil (BL52), Yoyang-gwan (GV3), Myeongmun (GV4), Hyeonchu (GV5), and Ashi (painful point) points. The needle retaining times for both groups were 15 mins.
The subjects were evaluated at the first visit and again at the first visit after the eighth treatment. To objectively evaluate the patients’subjective pain, we adopted a broadly-utilized measure, the visual analog scale (VAS) [12], which evaluates pain on a scale from no pain as 0 to unbearable pain as 10. The patient chooses a number to evaluate the pain level. We also used the pain rating scale (PRS) [13], which is based on a multilateral pain questionnaire created by joint research at Inje University and Yonsei University. It evaluates pain with several standards such as intensity of pain, number of times a day that pain occurs (frequency), dependence of pain on the aspects of motions, and the duration of pain. The following equation was used to obtain the PRS score (see Appendix 1): PRS score = intensity x (duration + frequency + motion)
As a final evaluation we used the Oswestry low-back pain disability index (ODI) [14], which is based on a multiple-choice questionnaire completed by the patient and which consists of 10 items related to daily-life activities. Each item describes an everyday-life activity in 6 steps from 0 to 5. This method has more meaning to evaluate the degrees of disability in everyday life than pain levels, showing functional conditions with numbers during the lumbago test. Ambiguous and inappropriate items, such as sexual activity, were omitted, so only nine items were included on the questionnaire (see Appendix 2).
Using the SPSS 18.0 for Windows for statistical processing, we considered results with
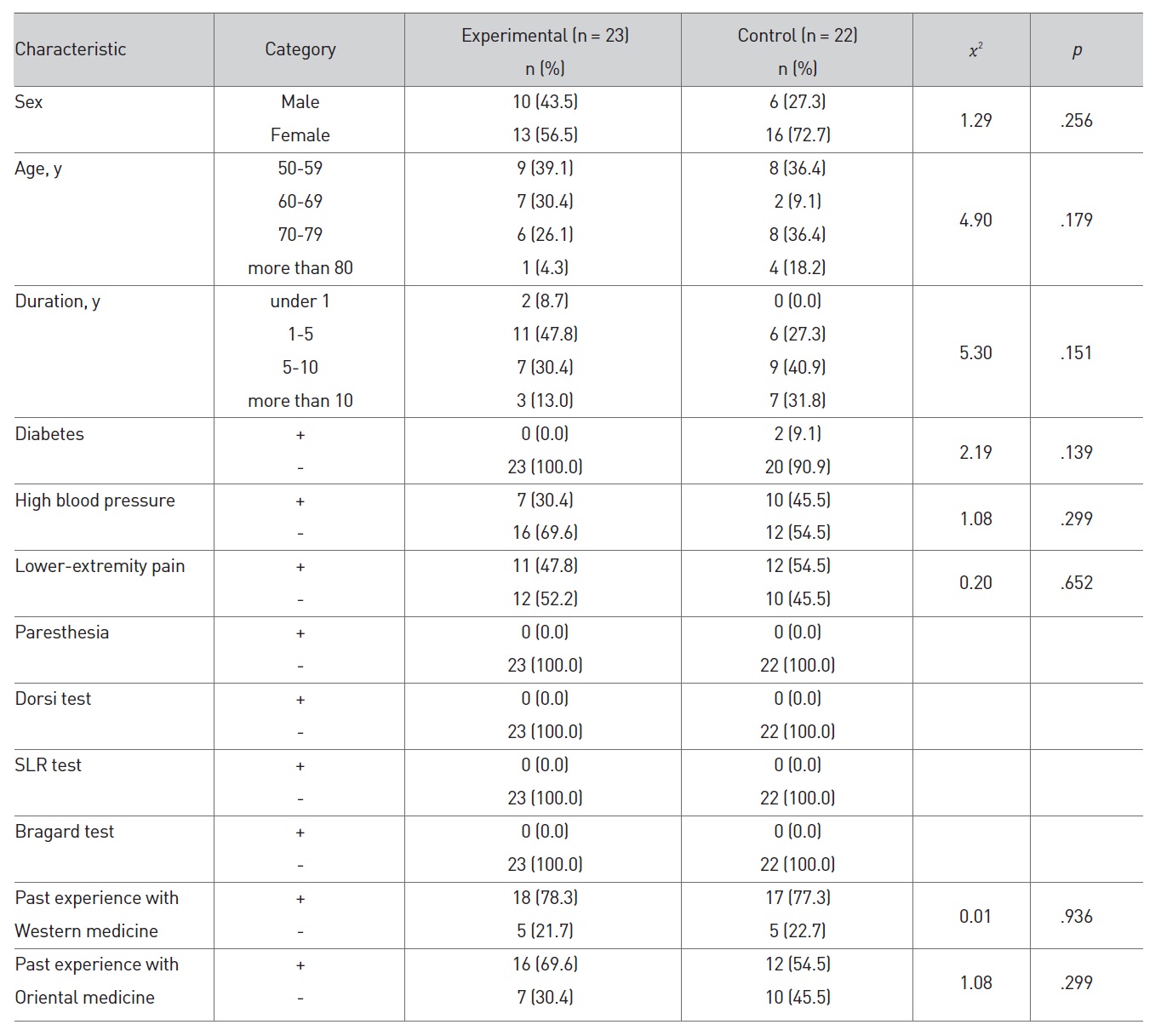
Testing of the homogeneity for the general traits and the disease- related characteristics between the experimental group and the control group showed no statistically meaningful differences between the two groups (see Table 1).
The mean values of the VAS, PRS and ODI for the experimental group were 7.17 ± 1.78, 53.04 ± 20.75, and 16.09 ± 5.99, respectively, and those for the control group were 7.05 ± 1.86, 56.64 ± 24.27, and 18.82 ± 5.15. No statistically meaningful differences were noted between the experimental group and the control group, indicating that the two groups were homogeneous. The homogeneity test results for the VAS, PRS, and ODI for both groups before the pharmacopuncture treatment are in Table 2.
The differences in the VAS values between pre-pharmacopuncture treatment and post-pharmacopuncture treatment were obtained for both the experimental and the control groups. The VAS value for the experimental group went down 3.35 ± 1.99 points from 7.17 ± 1.78 at pre-treatment to 3.83 ± 2.04 posttreatment, and the value for the control group went down 1.82 ± 2.11 points from 7.05 ± 1.86 to 5.23 ± 2.29. This difference showed statistical meaning (
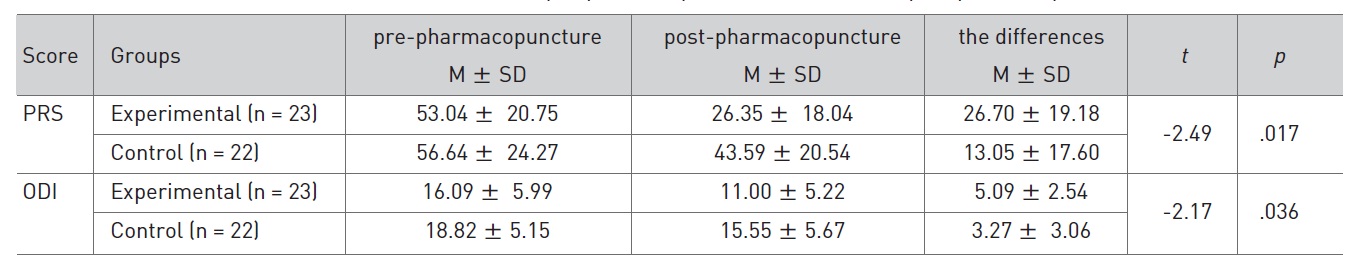
In addition, the differences in the PRS values between prepharmacopuncture treatment and post-pharmacopuncture treatment were obtained for both groups. The PRS value for the experiment group went down 26.70 ± 19.18 from 53.04 ± 20.75 at pre-experiment to 26.35 ± 18.04 at post-experiment, and the value for the control group went down 13.05 ± 17.60 from 56.64 ± 24.27 to 43.59 ± 20.54, a statistically-significant difference (
Finally, the differences in the ODI values between prepharmacopuncture treatment and post-pharmacopuncture treatment were obtained for both groups. The ODI values for the experimental group went down 5.09 ± 2.54 from 16.09 ± 5.99
at pre-experiment to 11.00 ± 5.22 at post-experiment, and the values for the control group went down 3.27 ± 3.06 from 18.82 ± 5.15 to 15.55 ± 5.67, a statistically meaningful outcome (
Lumbago is a clinical symptom that accompanied humans’ orthograde history. The attack rate has rapidly increased as human life has expanded and activities have become more frequent in modern times [15]. The lumbar spine is tenser and more subject to compression than the other parts of the backbone due to its weight bearing. Its broader range of motion and higher muscle development results in more frequent injuries and deformities. About 80% of the general population is well known to experience lumbago more than once in their lifetimes, so lumbago is the most common type of pain encountered in clinical practice and has been reported to occur in 20%-30% of humans [16].
The oriental treatment of lumbago is mainly conservative. The literature contains various treatment options, including herbal medicine, acupuncture, physical therapy, chuna manual medicine, electro-acupuncture treatment and exercise. Many pharmacopuncture therapies, such as body acupuncture, Sa-am acupuncture, Dong-Si acupuncture, eight-constitution acupuncture, auricular acupuncture, hand-finger acupuncture, and pharmacopuncture, are used in various combinations [4]. Pharmacopuncture is an oriental treatment method in which certain amounts of ingredients extracted from oriental medicine herb are injected into the meridian points or reaction points on the body’s surface after a diagnosis of the patient’s physical constitution and disease status has been established. This therapy has clinical advantages in exhibiting both acupuncture and drug effects [17].
The constituents of the Chukyu (spine-healing) pharmacopuncture are Cervi Parvum Cornu (deer antlers), Moschus (musk), Angelicae Gigantis Radix, Cnidii Rhizoma, Ostericii Radix, Angelicae Pubescentis Radix, Astragali Radix, and Scolopendra, which are extracted at low temperature and low pressure in an aseptic room at the Korean Pharmacopuncture Institute. Deer antlers have anti-arthritis effects [18], as well as analgesic effects [19]. Moschus has been reported to impact the immune response [20]. In addition, many studies have reported on the analgesic effects of Angelicae Gigantis Radix, Cnidii Rhizoma, Ostericii Radix, Angelicae Pubescentis Radix [21-24], and Astragali Radix has been shown to have an analgesic impact [25] on arthritis in animal models. Scolopendra has therapeutic effects on patients with herniated intervertebral discs of the lumbar spine [26] or cauda equine syndrome [27] through its anti-inflammatory activity [28].
Many researchers currently use pharmacopuncture therapy in patients with lumbago or skelalgia. Cha et al. [6], Yu et al. [7] and Lee et al. [8] performed a combination of acupuncture therapy and bee venom pharmacopuncture on patients with herniation of the lumbar intervertebral discs. They suggest that bee venom pharmacopuncture had a significant effect on the disease. Yoon et al. [9] confirmed the effects of Carthami Flos pharmacopuncture on lumbago patients. Lee et al. [10] showed that bee venom pharmacopuncture and Jungsongouhyul pharmacopuncture, either alone or in combination, had an impact on patients with lumbago or skelalgia.
In spite of several investigations regarding the effects of pharmacopuncture on lumbago and skelalgia, whether its curative effects are attributed to pharmacopuncture effects, psychological effects or a natural course is controversial. Based on the results of Seo and Xue [11], we conducted a comparative study of Chukyu (spine-healing) pharmacopuncture and saline (normal saline; NS) pharmacopuncture. We conducted a randomized, controlled trial that included 45 patients who visited the acupuncture & moxibustion department at Dong-Eui University Hospital of Oriental Medicine for lumbago and skelalgia from July 5, 2011 to January 31, 2012.
The VAS for the Chukyu (spine-healing)-pharmacopuncture group (experimental group) fell 3.35 ± 1.99 points from 7.17 ± 1.78 pre-experiment to 3.83 ± 2.04 post-experiment and, that for the saline-pharmacopuncture group (control group) decreased 1.82 ± 2.11 points from 7.05 ± 1.86 to 5.23 ± 2.29, a statistically meaningful result (
This study included 45 subjects who visited the acupuncture & moxibustion department at Dong-Eui University Hospital of Oriental Medicine from July 5, 2011, to January 31, 2012. Their chief complaint was lumbago and skelalgia. To evaluate the medical effects of Chukyu (spine-healing) pharmacopuncture, we analyzed the VAS, PRS and ODI and reached the following conclusions:
(1) The VAS in the Chukyu (spine-healing)-pharmacopuncture treated group showed more statistically significant differences than it did in the saline pharmacopuncture treated group.
(2) As to the level of pain (degree, frequency, motion, duration) measured by using the PRS, the Chukyu (spine-healing) pharmacopuncture treated group showed more statistically meaningful differences than the saline pharmacopuncture treated group.
(3) As to the degree of disability in daily life measured by using the ODI, the Chukyu (spine-healing) pharmacopuncture treated group showed more statistically significant differences than the saline pharmacopuncture treated group did.
>
Appendix 1: Questionnaire for Determining the Value on the Pain Rating Scale
To determine the value on the pain rating scale, we asked each patient to answer the questions below and used the following equation: PRS rating scale = intensity of pain x (time + frequency + movement).
□ What is the level of pain? (intensity of pain)
10. Cannot even bear the moment without taking some measures right on the spot
9. Cannot stand still and become overwhelmed by pain
8. Frown, groan, and cannot move at all from pain
7. Not that much groaning but frowning
6. Not that much frowning but cannot focus on other things
5. Can do other things by suppressing the pain, but the pain still bothers me
4. Can suppress pain but still bothers me
3. Some pains but can forget it by concentrating on other things
2. Sometimes the pain is felt, but it is usually out of mind
1. Not much pain, but not completely well
0. Perfectly fine; no pains at all
□ How long does the pain last once it occurs? (time)
5. Pain goes over 10 hrs at one time
4. About 5 to 10 hrs at one time
3. About 2 to 5 hrs at one time
2. About 15 mins to 2 hours at one time
1. Less than 15 mins at one time
□ How many times does the pain arise a day? (frequency)
5. Feel pain constantly all day
4. Feel pain more than 2 times a day
3. Feel pain more than once a day
2. Feel pain 2-3 times a week
1. Feel pain once or less a week
□ What about the dependence of the occurrence of pain on movement (the aspects of pain related to actions)? (movement)
5. Feel pain when even in stable condition
4. Feel pain even when slightly moving
3. Feel pain when moving lightly in ordinary daily life
2. Feel pain when moving a bit more than normal
1. Feel pain when taking intense action or exercise
0. No pain with any movement or actions
>
Appendix 2: Oswestry Low-back Pain Disability Index
Each patient was asked to answer the following questions:
1. How is the level of pain?
0. Small pain that comes and goes
1. Little pain, but not much.
2. Moderate pain, but bearable
3. Intense pain that needs to be treated
4. Too much pain to bear even after treatment
5. Too much pain to live daily life
2. How much help do you need?
0. No problem moving
1. No problem moving, but pain follows
2. Need to move slowly and carefully because of discomfort
3. Need to get some help to move, but can do other normal things alone
4. Need to get help to move
5. Totally cannot move.
3. What about picking thing up?
0. Can carry heavy items without any help
1. Can pick up heavy items, but pain follows
2. Cannot pick up items on the floor because of pain
3. Cannot pick up items on the floor, but can carry items at a certain height.
4. Can only carry light items
5. Cannot carry anything
4. How is it to walk around?
0. No problem walking around
1. Cannot walk over 1 hour due to pain
2. Cannot walk over 30 mins due to pain
3. Cannot walk over 10 mins due to pain
4. Can barely walk with a cane or a walking frame
5. Spend most time lying down and hard to go to bathroom
5. How is the pain when sitting?
0. Can sit on anything anywhere for as long as desired
1. Can sit long enough on a comfortable chair
2. Cannot sit for over an hr due to pain
3. Cannot sit for over 30 mins due to pain
4. Cannot sit for over 10 mins due to pain
5. Cannot even sit at all due to pain
6. How is the pain when standing?
0. Can remain standing for as long as wanted
1. Can stand as long as desired, but pain follows
2. Cannot stand for over an hour due to pain
3. Cannot stand for over 30 minutes due to pain
4. Cannot stand for over 10 minutes due to pain
5. Cannot stand at all due to pain
7. How is the pain when sleeping?
0. No problem sleeping
1. Wake up once a night due to pain
2. Wake up 2-3 times a night due to pain
3. Wake up 3-5 times a night due to pain
4. Wake up frequently during the night due to pain
5. Cannot sleep due to pain
8. How is the pain in social life?
0. No problem in keeping a social life
1. Can do normal social activitieswithout pain occurring
2. Pain is not enough to be constrained except for intense activities
3. Pain limits social activities
4. Can barely do any social activities
5. Cannot do social activities at all due to pain
9. How are outdoor activities?
0. No problem going outside
1. Outdoor activities are followed by pain
2. Cannot continue outdoor activities for more than 2 hrs due to pain
3. Cannot continue outdoor activities for more than 1 hour due to pain
4. Cannot continue outdoor activities for more than 30 mins due to pain
5. Almost always at home due to pain