Neurofibromatosis type 1 (NF1), known as Von Recklinghausen disease, is one of the most common gene disorders to human. It has an incidence of 1 per 3,500 – 4,000 live births and its incidence among females is the same as that among males. NF1 is an autosomal dominant disorder caused by a mutation of a gene located on chromosome 17 [1]. According to the criteria for NF1 established by the National Institute of Health, the diagnosis of NF1 requires the presence of two or more of the following major criteria [2, 3]:
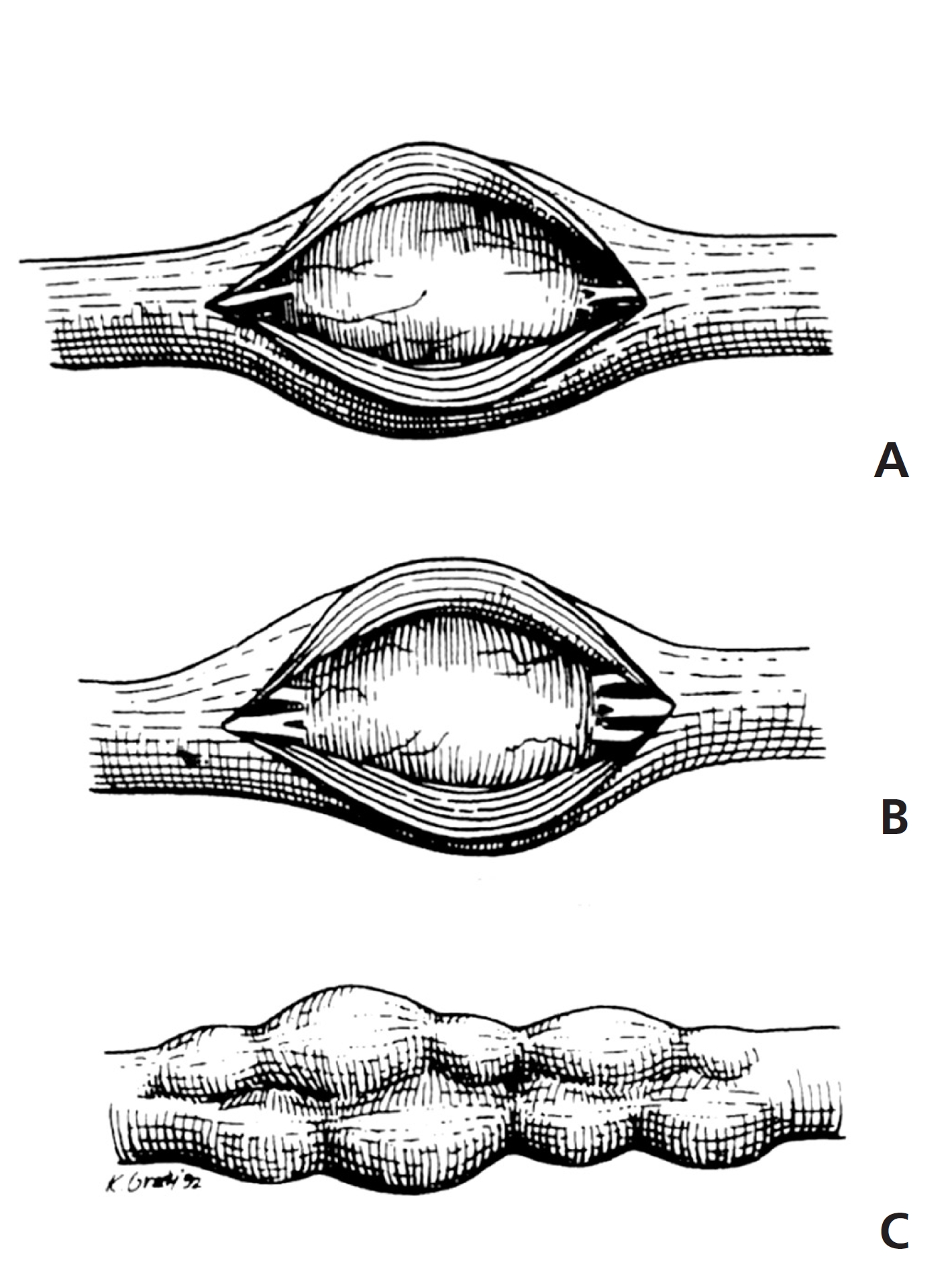
A plexiform neurofibroma (PNF) is a benign nerve tumor resulting from aberrant growth of the cells of the nerve sheath. It is composed of schwann cells, perineurial-like cells, and fibroblasts, originates from the central aspect of the nerve, and involves multiple fascicles. Although the fascicles are usually preserved, a diffusely-enlarged, thickened, irregular, and tortuous nerve is produced. Its morphologic appearance is classically compared to a “bag of warms” or “rosary beads” (Fig 1) [4-7]. It occurs in 25% – 30% of NF1 patients, with the growth rates and patterns of PNFs varying to a large extent and their growth spurts being unpredictable. Due to the large sizes of the tumors and the involvement of multiple fascicles of nerves and tissues, the risk of neurological and functional destruction upon tumor resection is high. Thus, surgical interventions are commonly postponed as long as possible. In addition, most surgical interventions are limited to debulking, so the remaining tumors often re-grow, leading a need for repeated interventions [8, 9]. There have been no reports on PNFs or on NF1 in traditional Korean medicine. Here, we report a case of a teenage girl with PNFs in the pelvic region who was treated by using sweet bee venom (SBV) and mountain ginseng pharmacopuncture (MGP) for 4 years.
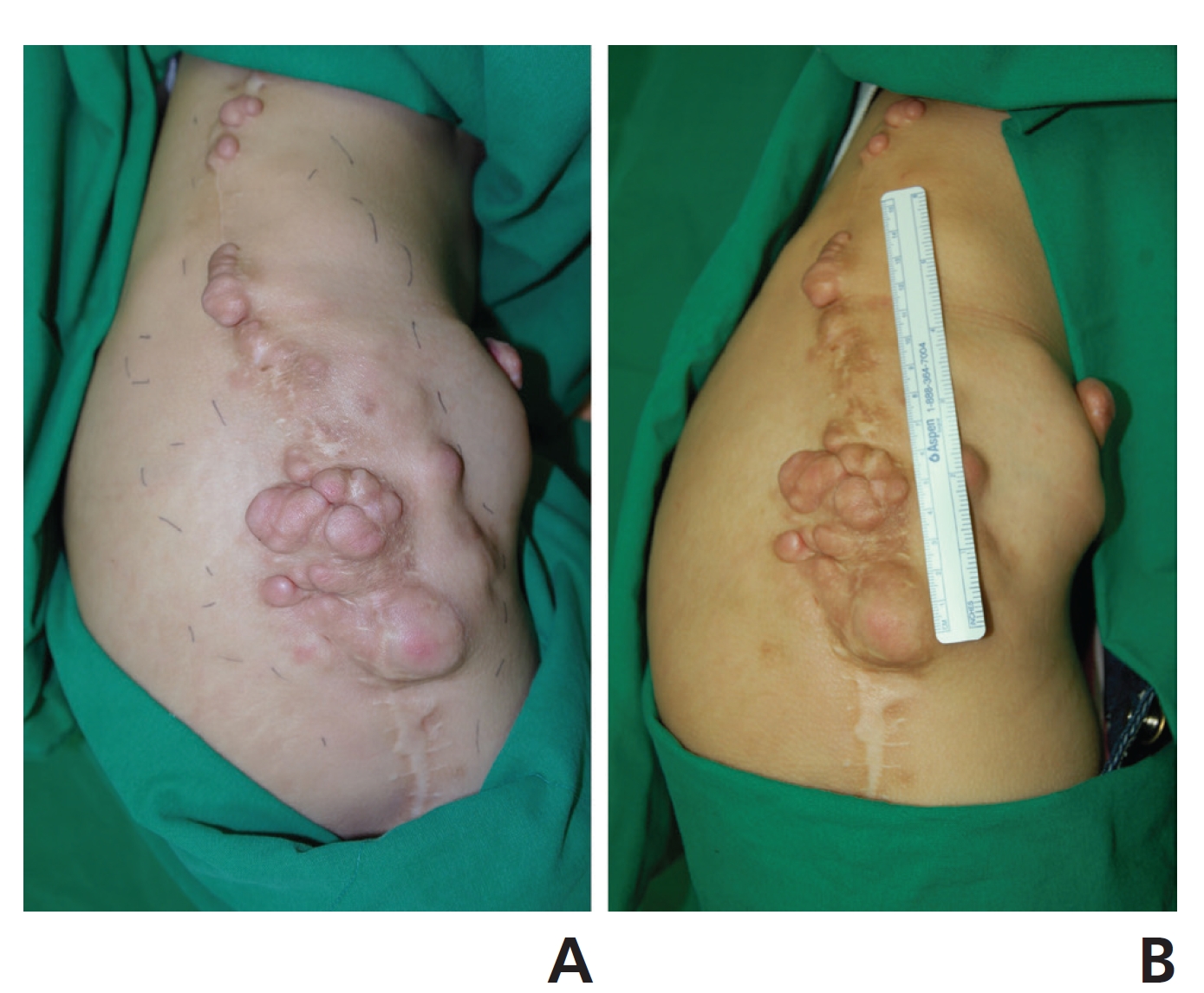
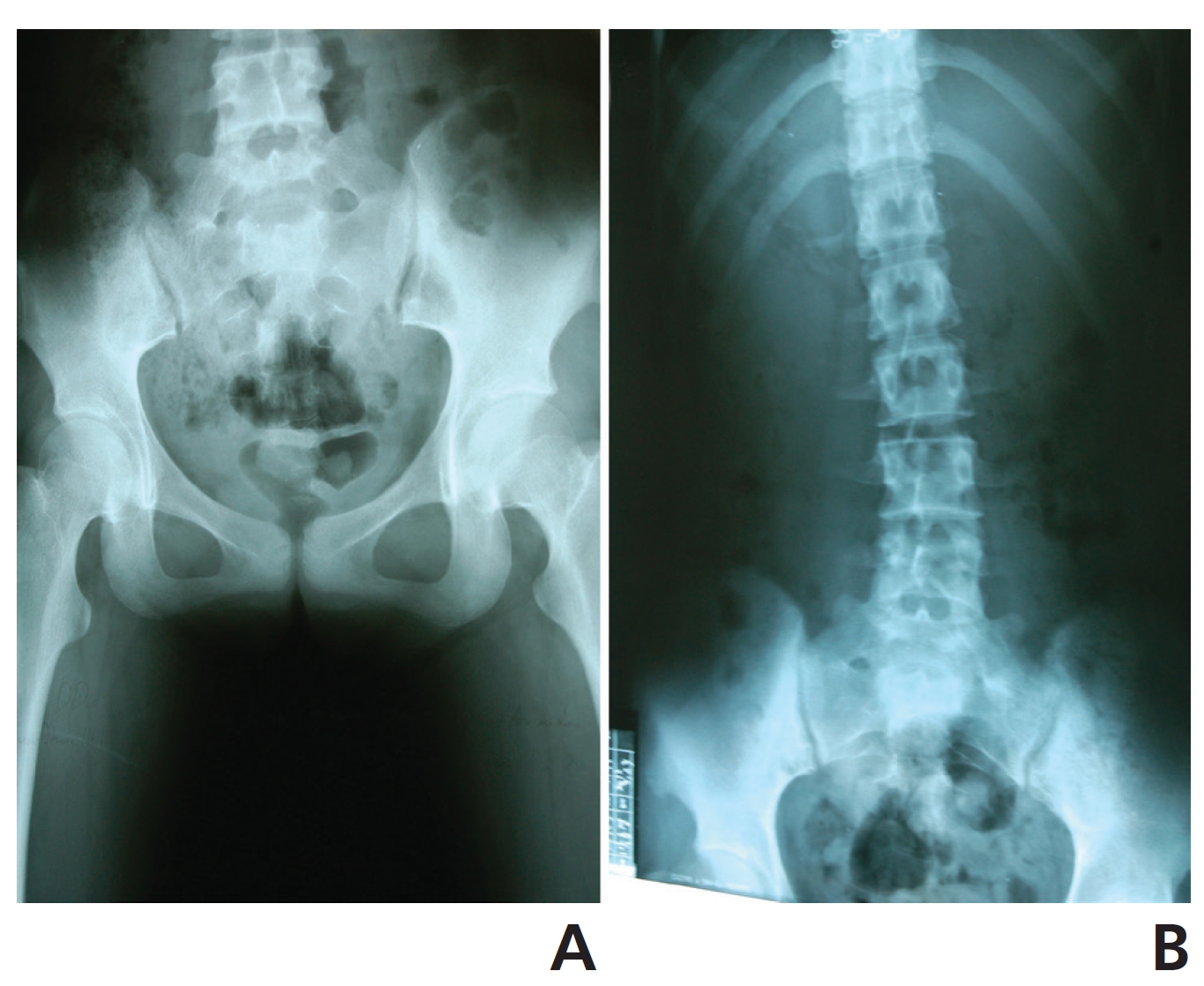
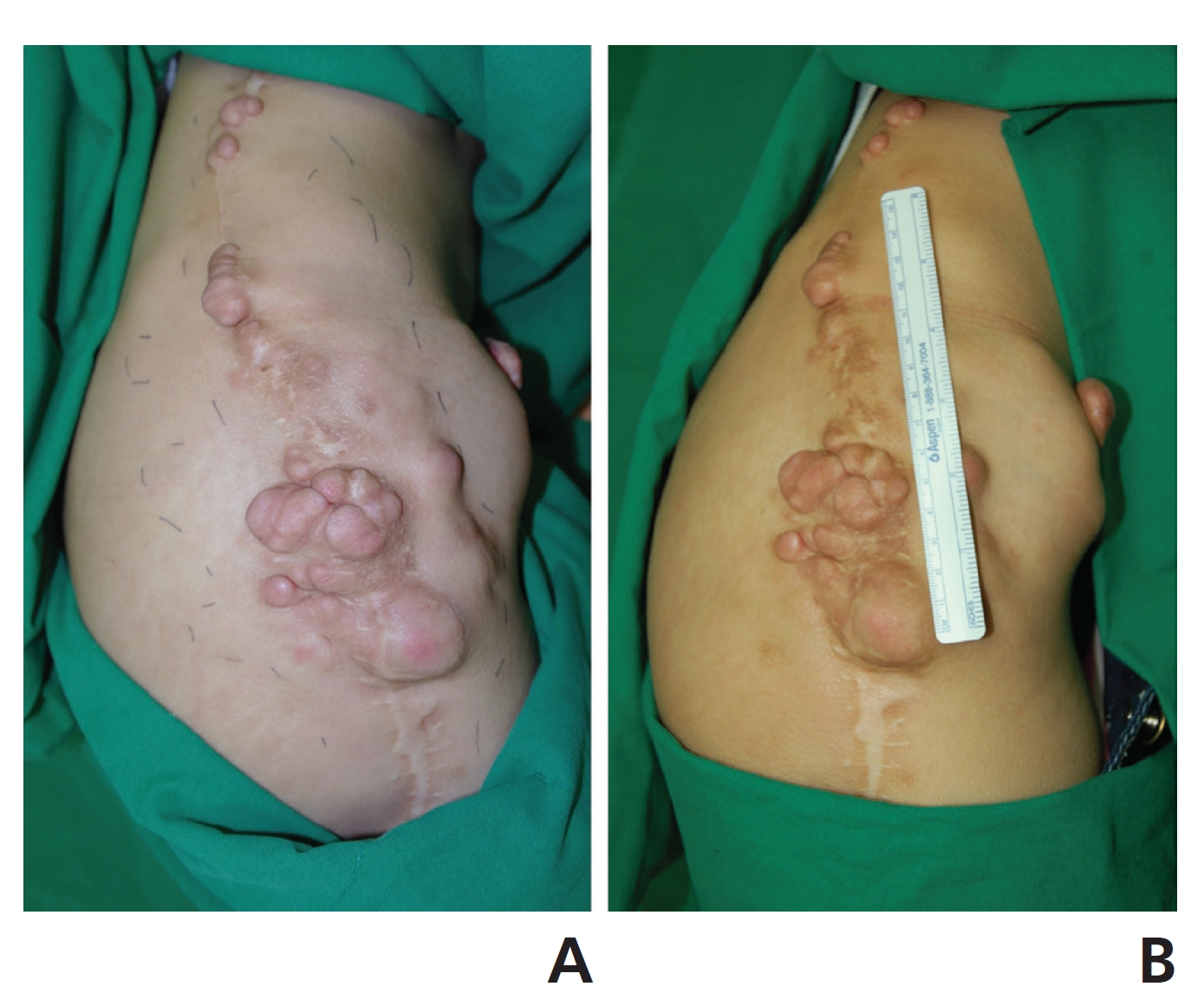
A 16-year-old girl visited our clinic with PNFs in March 2010. She had been diagnosed with PNFs in NF1 10 years earlier and had had surgery to remove the benign tumors three times at a general hospital in Seoul during her first 4 years of treatment at that hospital. Although she had undergone surgery, the re-growths of the PNFs occurred rapidly, so her family wanted to consider the use of alternative medicines. She had multiple subcutaneous fibromatoses (30 cm × 20 cm) in the right hip joint and pelvic region, subcutaneous nodules (1 cm × 5 cm) in the left hip joint, and limited range of motion in the right hip joint (Fig 2). The L-spine and pelvic X-rays showed only low-grade scoliosis, no bones had been affected by fibromatosis (Fig 3). She also showed symptoms of general weakness, coldness of the hands and the feet, and skin rashes.
The patient and her family signed an informed consent form, and this case was approved by Institutional Review Board of the Korean Medicine Hospital of Sangji University.
SBV was administrated intracutaneously at the borders of the PNFs in the pelvic regions in a dose of 5 mL every two weeks. We used SBV produced by the Korean Pharmacopuncture Institute and 1-mL syringes (26 G × 13 mm, Sungshim Medical Co., Bucheon, Korea) were used for SBV. Also MGP (Korean Pharmacopuncture Institute, Seoul, Korea) was injected intravenously in a dose of 20 mL every two weeks using syringes (23 G × 25 mm, 20 mL, CPL Co., Ansan, Korea). We performed no treatments other than the treatment using SBV and MGP.
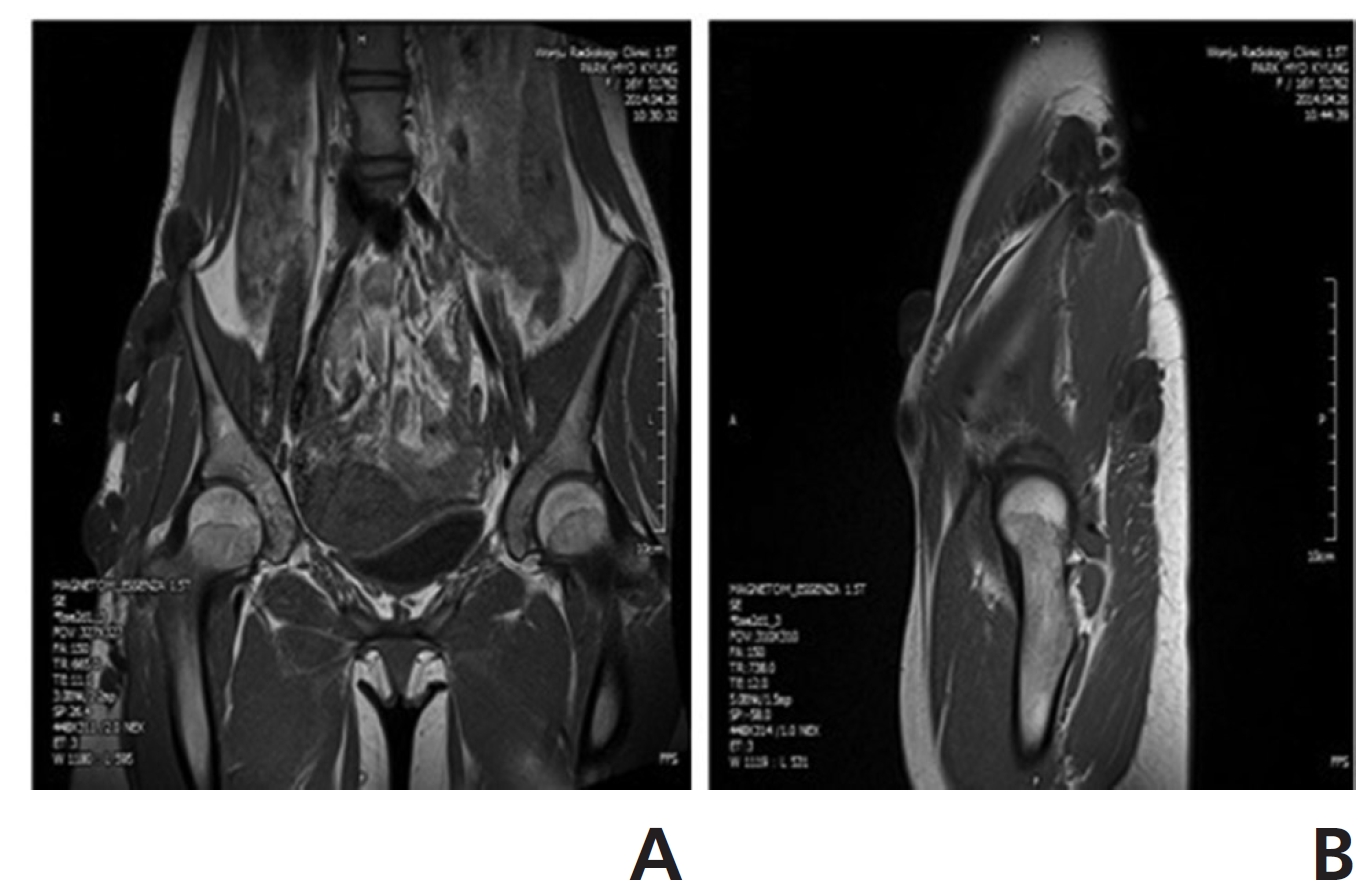
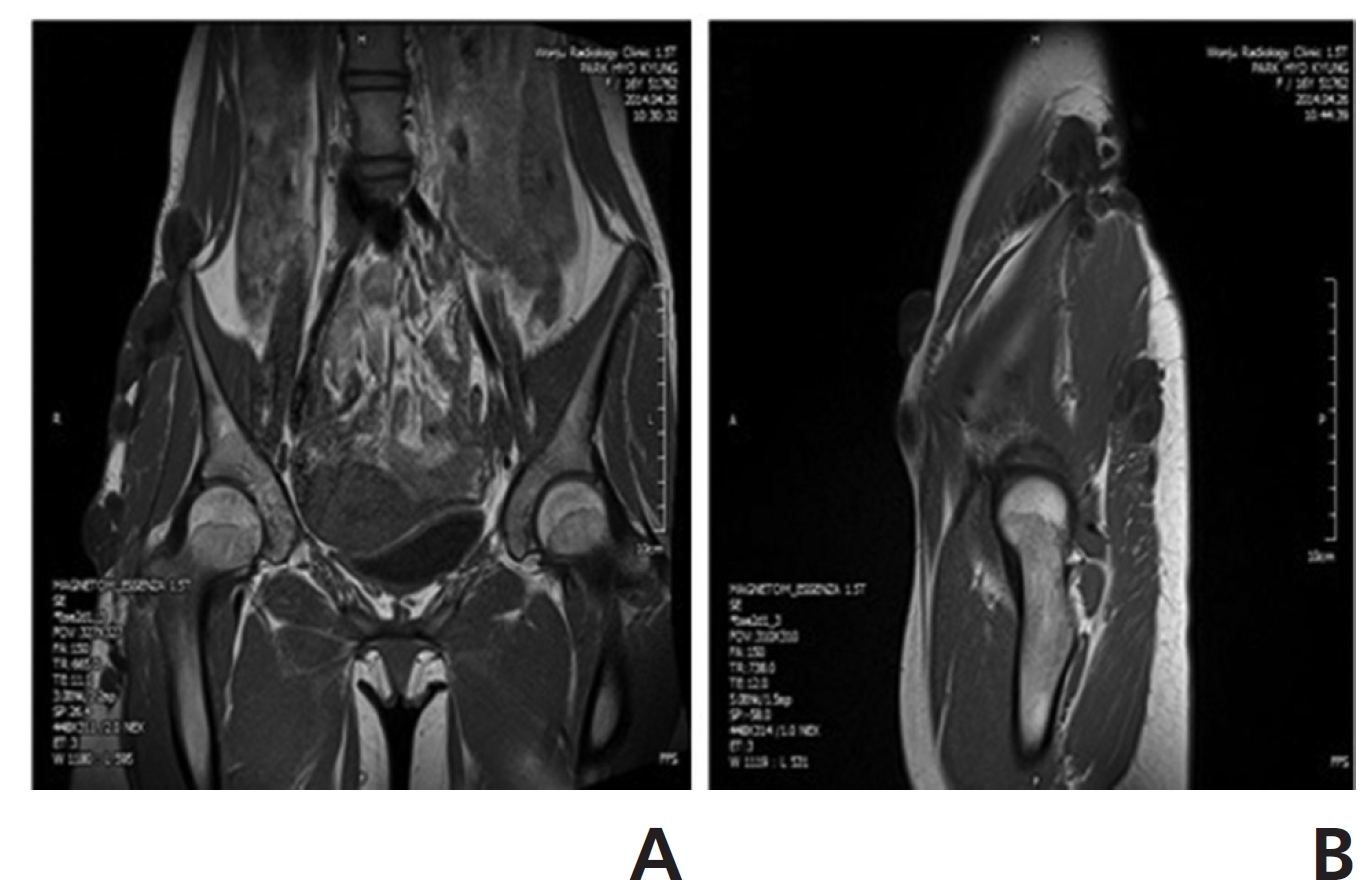
From March 2010 to April 2014, her tumors almost stopped growing and showed only a few changes. Also, the range of motion in her right hip joint and her general condition improved. magnetic resonance imaging (MRI) in April 2014 to check if bones or organs had been affected showed that the fibromatosis remained subcutaneous and that no bones or organs had been affected (Fig 4).
PNF is a benign tumor that spreads either just under the skin (superficial) or deeply in the body, and 25% – 30% of NF1 patients suffer from PNFs. PNF patients have functional impairment and cosmetic problems. PNF is histologically characterized with proliferation of the schwann cells in the nerve sheath, involving multiple fascicles and multiple nerves throughout the nerve involved. It occurs frequently in the head and neck region due to the rich nerve innervation; however, it also appears on rare occasions in the extremities. Although PNFs are benign, they have a 2% – 5% potential for malignant transformation [4- 12].
This patient presented with PNF masses in the right pelvic region when she was 6 years old and was diagnosed as having PNFs in NF1 at a general hospital in Seoul. Because of the rapid growths of the fibromatosis, her hip joint pain, and limited her rage of motion, she underwent surgery three times. However the growth continued, and new nodules were observed in her left hip joint. Since the patient has undergone treatments every 2 weeks with SBV and MPG in our clinic.
Her PNFs have not grown since she began being treated in our clinic in March 2010. Generally, a higher dosage BVP is considered for severe disorders. If a patient experiences no adverse reactions to BVP, the dosage may be increased to 50% BVP. However, BVP always has a risk of allergic responses, so we used SBV. SBV is associated with fewer allergic responses than BVP is, so SBV makes it possible to use high dosage from early stage of treatment on severe patients [13]. We used a dose of 5 mL every treatment, which is a very high dosage. MGP has effects of anti- cancer and stimulates immune system [13], so we think that the high doses of both SBV and MGP helped to maintain her good condition.
Because no changes of tumor size have been observed and she is reaching adolescence, she wants another surgery on the fibromatosis region. A complete resection is often difficult due to the extensive growths of the tumors and invasion of the surrounding tissues, and re-growth after surgery is common. Also, PNFs have unpredictable patterns of growth, which can cause confusion. Surgical interventions are, thus, commonly postponed as long as possible [4-6]. For these reasons, we advised her and her family to delay surgery until she reaches an age at which she is considering-marriage.
The MRI technique can be used to determine the diagnosis, morphology, type and size of lesion, and extent of disease and to differentiate superficial PNFs from other very similar lesions, such as lymphatic or venous malformations and hemangiomas. Especially, MRI helps to differentiate a PNF from a malignant peripheral nerve sheath tumor [10]. In our case, MRI revealed multiple masses of fibromatoses subcutaneously from the right iliac crest to the hip joint; however, no bones or organs were affected, and no malignancies were observed.
Growth of a PNF can occur at any time in life, and a PNF has an unpredictable pattern of growth. PNFs tend to grow during times of hormonal change, such as early childhood, puberty, or pregnancy, and then, in some cases, stop entirely [4, 14]. Thus, further studies and long-term tracking observations of this patient are needed in order to confirm whether SBV and MGP treatment was effective in this case.
We think SBV and MGP treatment has effects that have suppressed the growth and the spread of the PNF in this patient. Further studies are needed to confirm the effects of SBV and MGP treatment on a PNF.

![The difference in shape between benign neural sheath tumors:
(A) schwannoma (B) neurofibroma and (C) plexiform neurofibroma
[7].](http://oak.go.kr/repository/journal/13155/DHOCBS_2014_v17n3_74_g001.jpg)