The high-dose-rate (HDR) brachytherapy technique recently replaced low-dose-rate (LDR) brachytherapy procedures for various reasons, including the fact that the treatment time is shorter and patient hospitalization is no longer necessary. The International Commission on Radiation Units and measurements (ICRU) Report 38 classifies HDR brachytherapy techniques as those that deliver very high dose rates (20cGy/min or more)1). This means that any mistakes made during HDR treatment could have significant consequences. Thus, the safety of HDR brachytherapy treatment units should be stringently ensured.
In Korea, a statistical study by the Korean Society for Therapeutic Radiology and Oncology showed that, in 2006, 1,561 of 37,215 (4.2%) radiation oncology patients received brachytherapy primarily in order to treat intracavitary tumors.2) Thus, far fewer radiation oncology patients undergo brachytherapy treatments compared to those who undergo external beam radiation therapy (EBRT). Nevertheless, shielding for brachytherapy units remains a crucial consideration when installing or remodeling brachytherapy facilities. The National Council on Radiation Protection and Measurements (NCRP) reports provide guidelines with regard to shielding design and documentation of radiation safety reports for radiation therapy units. NCRP Report 49, which was published in 1988, provided suitable broad-beam tenth value layer shielding data as well as suitable exposure rate constants for several radioisotopes, including Iridium-192 which is the most common radioisotope used in current HDR brachytherapy practice.3) NCRP Report 151 suggests a suitable weekly treatment time for brachytherapy equipment.4) In Korea, the Korea Institute of Nuclear Safety is the regulatory agency that regulates nuclear safety matters, including radiation oncology facility planning or remodeling. This agency has established a guideline that radiation oncology departments can refer to when completing radiation safety reports. However, it is a general guideline for all radiation treatment equipments that focuses mainly on linear accelerator-based radiation therapy. Due to the different characteristics of radiation treatment equipments, individual guidelines for each type of treatment equipment may be needed for completing the radiation safety reports.
The present study evaluated 38 radiation safety reports for brachytherapy equipment to determine the current status of the brachytherapy units in Korea and the quality of the radiation safety reports that were completed by the radiation oncology departments. The results support the notion that standard guidelines specific for brachytherapy treatment are needed in order to complete radiation safety reports that reflect the current clinical situation of radiation oncology departments in Korea.
Of the 39 brachytherapy units that are currently operating in Korea, radiation safety reports were available for 38. The following data was collected from these radiation safety reports: radiation safety report publication year, brachytherapy unit manufacturer/supplier, type of sources used, activity of the source, availability and affiliation of the person who completed the report, exposure rate constant, the treatment time that was used to calculate workload, and the half-value-layer (HVL) values that were used to calculate the shielding design goal values. The number of radiation safety reports that were published each year was evaluated to determine the frequency of new brachytherapy equipment installation or remodeling. Brachytherapy unit manufacturer data and the radioisotope sources and their activity were sorted and percentages were obtained to determine trends in the use of brachytherapy techniques in terms of dose rates. Whether the persons who completed the report indicated their affiliations and whether they were affiliated with the institution or outsourcing companies were also determined. To determine how well radiation oncology departments in Korea completed the radiation safety reports, the exposure rate constants and treatment times per week that were used for calculating workload and shielding design goal values were assessed along with the HVL values that were used to evaluate shielding safety. Descriptive statistics were used to evaluate the current status of brachytherapy equipment in Korea and identify trends in radiation safety report completion.
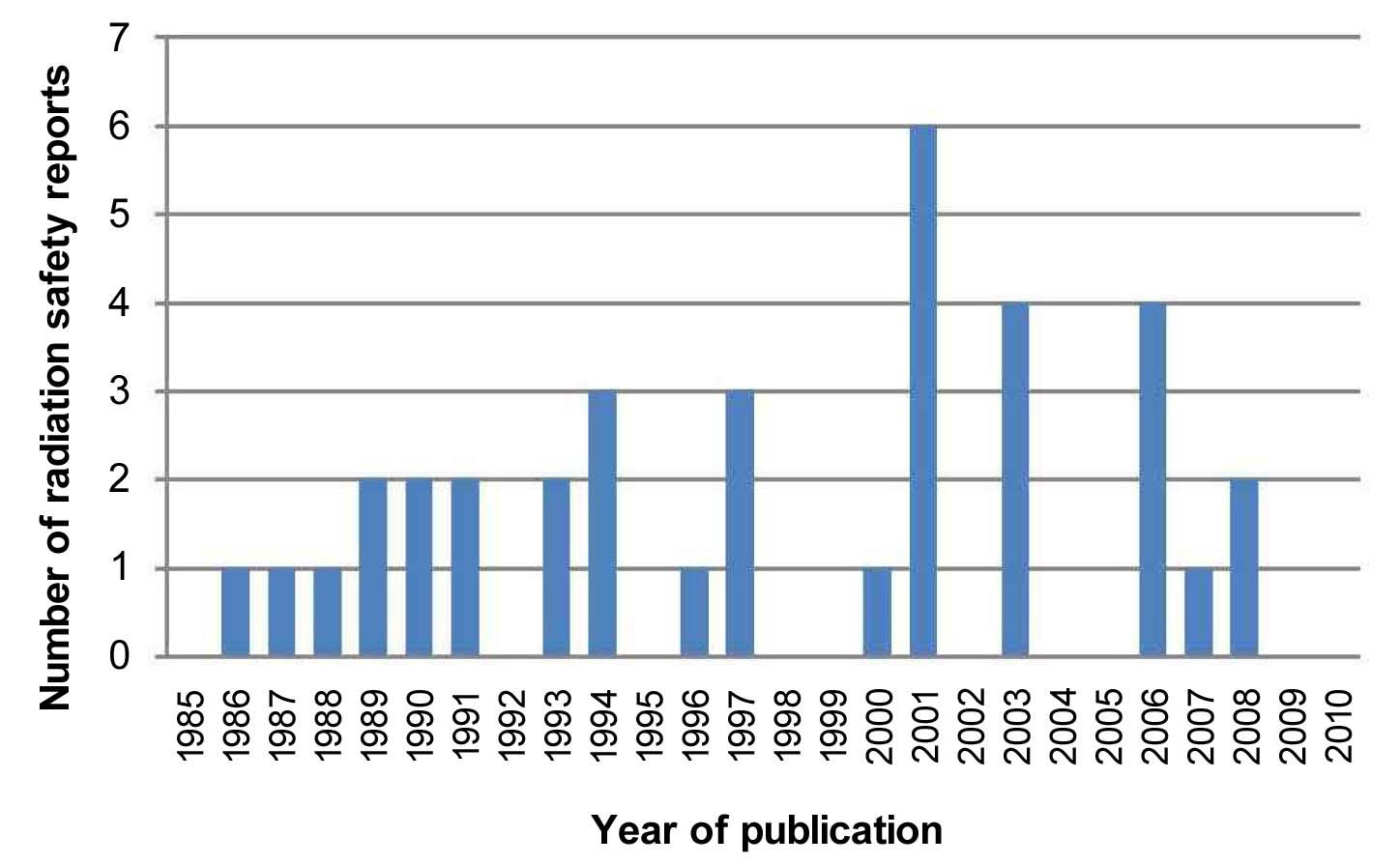
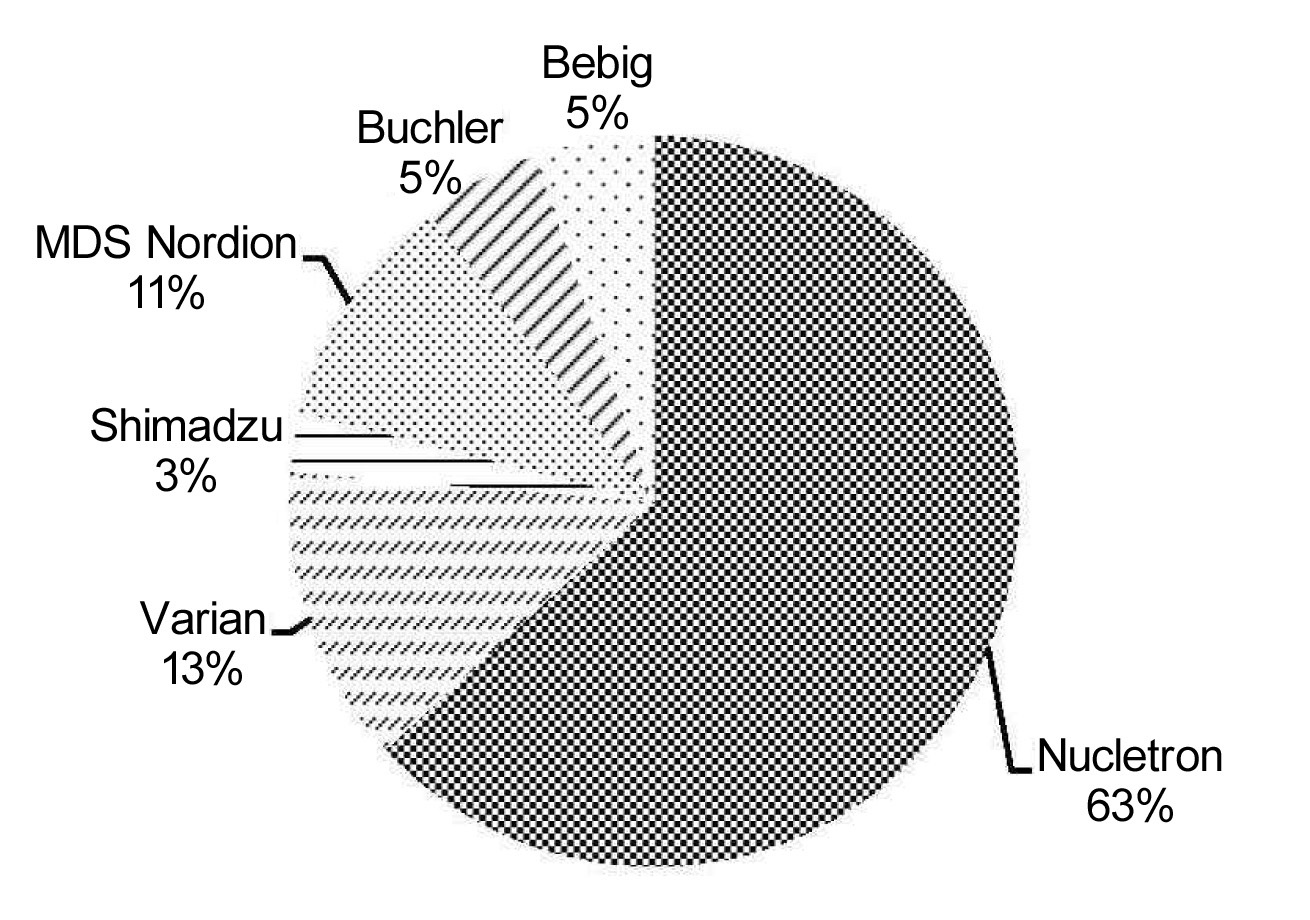
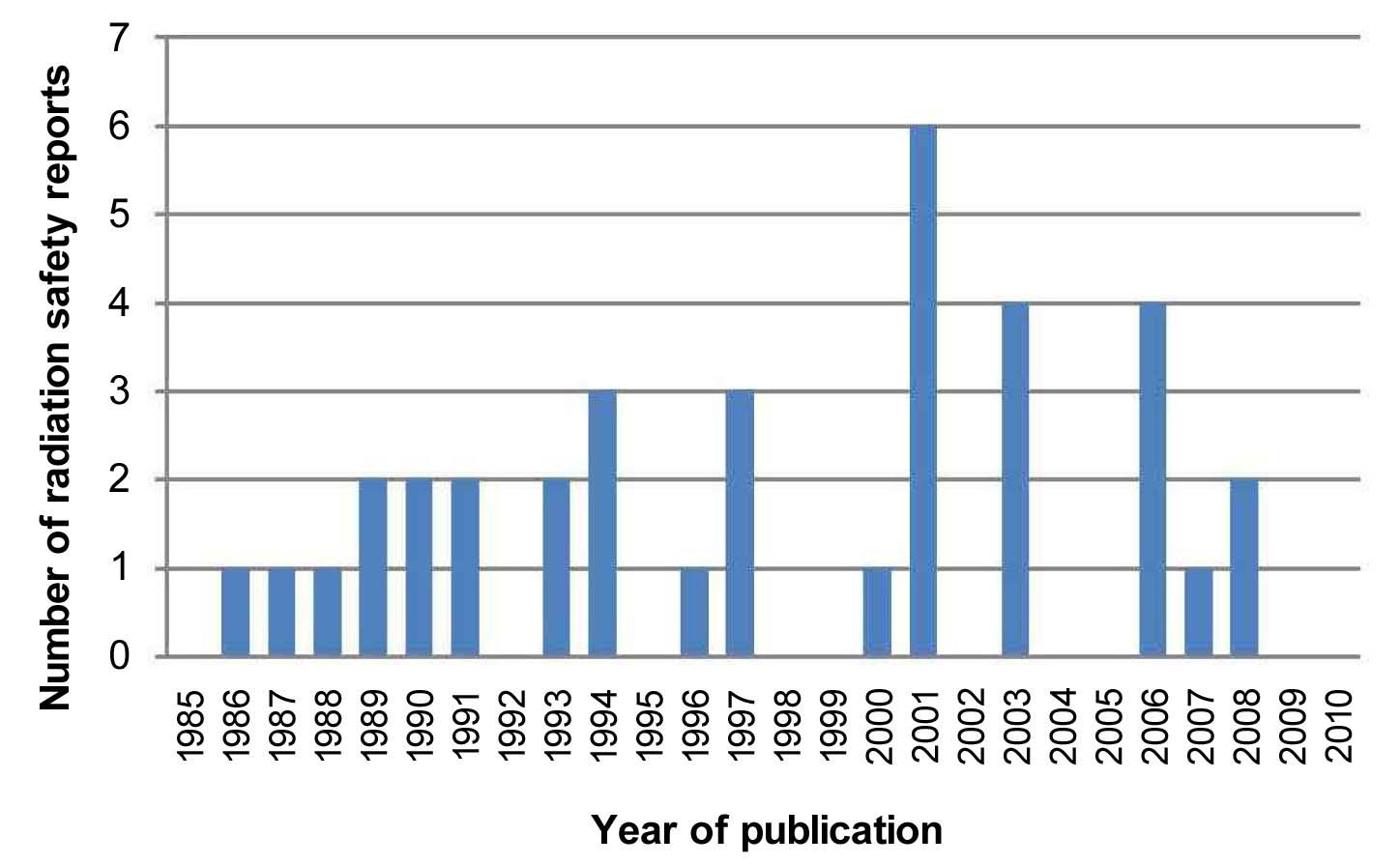
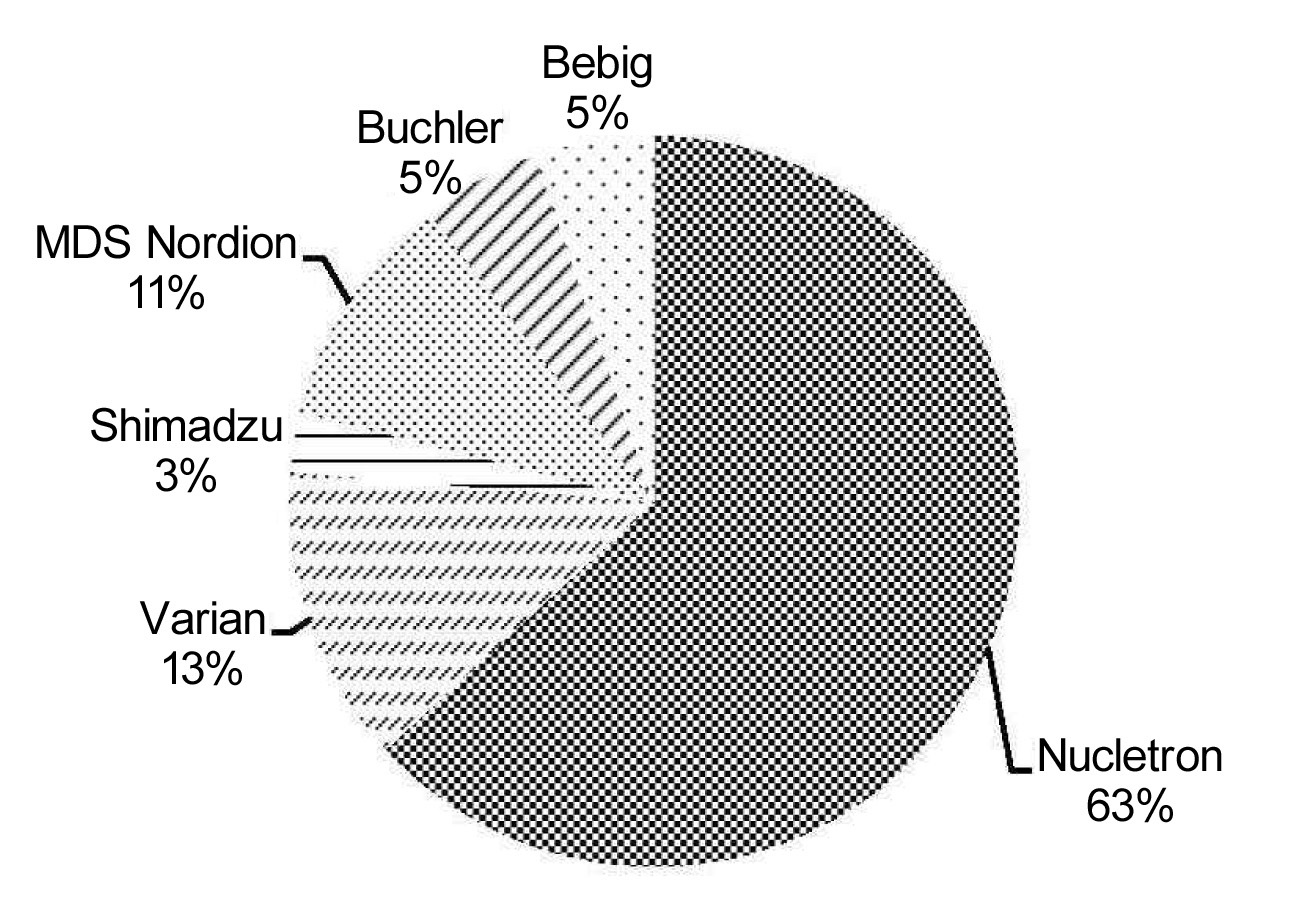
As shown in Figure 1, radiation safety reports were published at a fairly constant rate over the period of 1985 and 2010, which was when current brachytherapy units in Korea were installed. There was an exceptional burst of reporting in 2001. Table 1 shows that six different manufacturers supplied brachytherapy units to oncology departments in Korea, namely, Nucletron, Varian, MDS Nordion, Buchler, Bebig and Shimadzu. As shown in Figure 2, Nucletron supplied most of the brachytherapy units (63.2%), followed by Varian (13.2%), MDS Nordion (10.5%), Bebig (5.3%), Buchler (5.3%) and Shimadzu (2.6%). It should be noted that, in 2002, Varian Medical Systems, Inc. acquired the HDR brachytherapy business of MDS Nordion, and two of the five equipments supplied by Varian after 2002 were actually the GammaMed model of MDS Nordion.
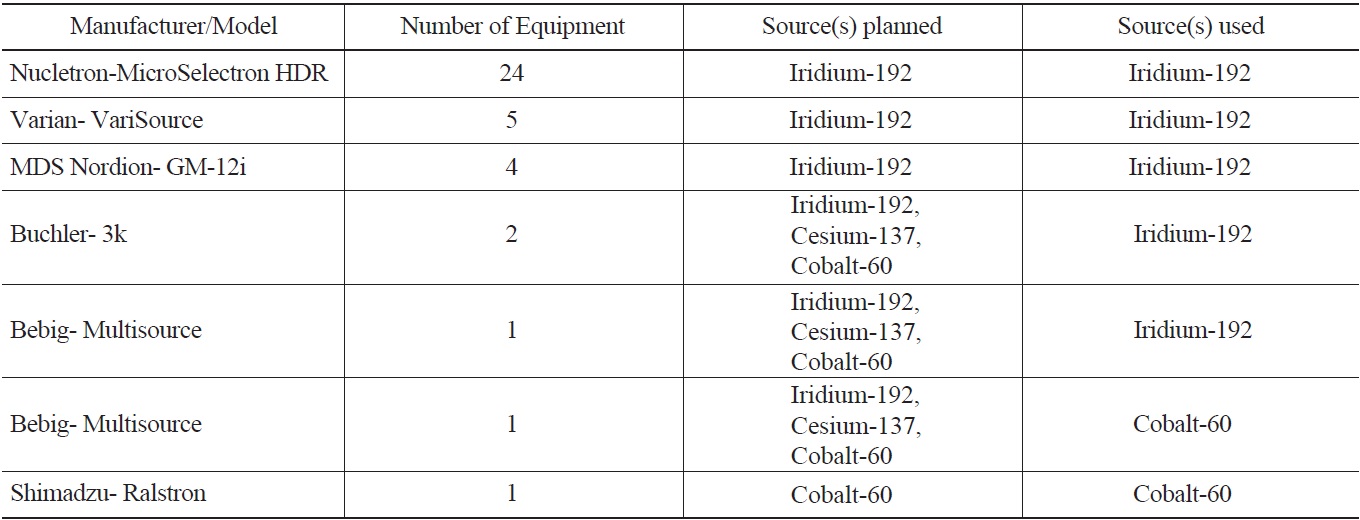
In total, 33 institutions utilized HDR brachytherapy techniques with units from Nucletron (N=24), Varian (N=5) and MDS Nordion (N=44) that used Iridium-192 sources (Table 1). Four institutions employed units that used three interchangeable sources (Cobalt-60, Cesium-137 and Iridium-192). These units were supplied by Buchler- 3K (N=2) and Bebig-MultiSource (N=2). One institution used a HDR brachytherapy unit from Shimadzu-Ralstron, which employed a Cobalt-60 source.
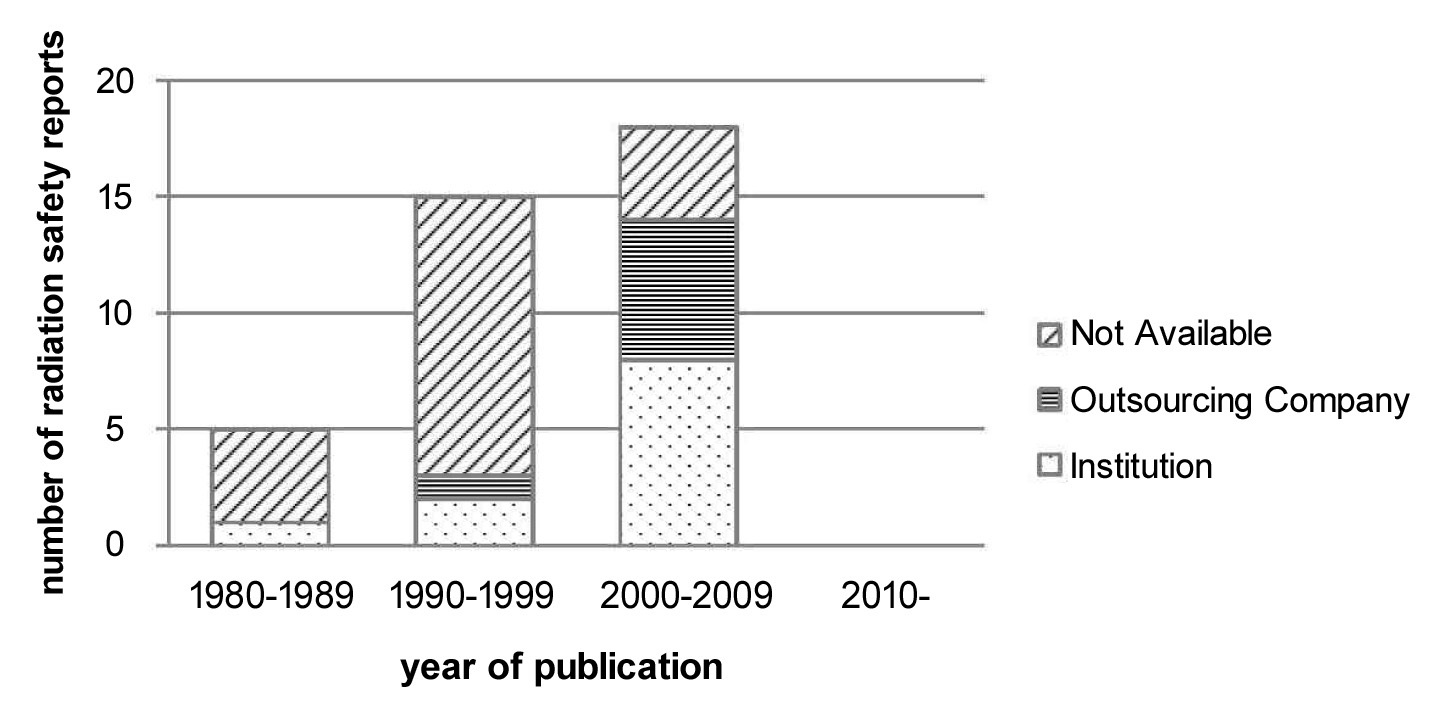
The Nuclear Safety and Security Commission as well as international guidance setting bodies such as the NCRP state that the radiation safety report must include the personal information and qualifications (education, training, and experience) of the person who performed the survey and completed the report.4, 5) In the present study, 47.4% of the radiation safety reports complied with these regulations by including the personal information of the drafter. Of the 38 reports, 11 (28.9%) were processed by an applicant who was affiliated with the institution itself, seven (18.4%) were processed by an outsourcing company, and the remaining 20 reports (52.6%) failed to include the personal information of the drafter.
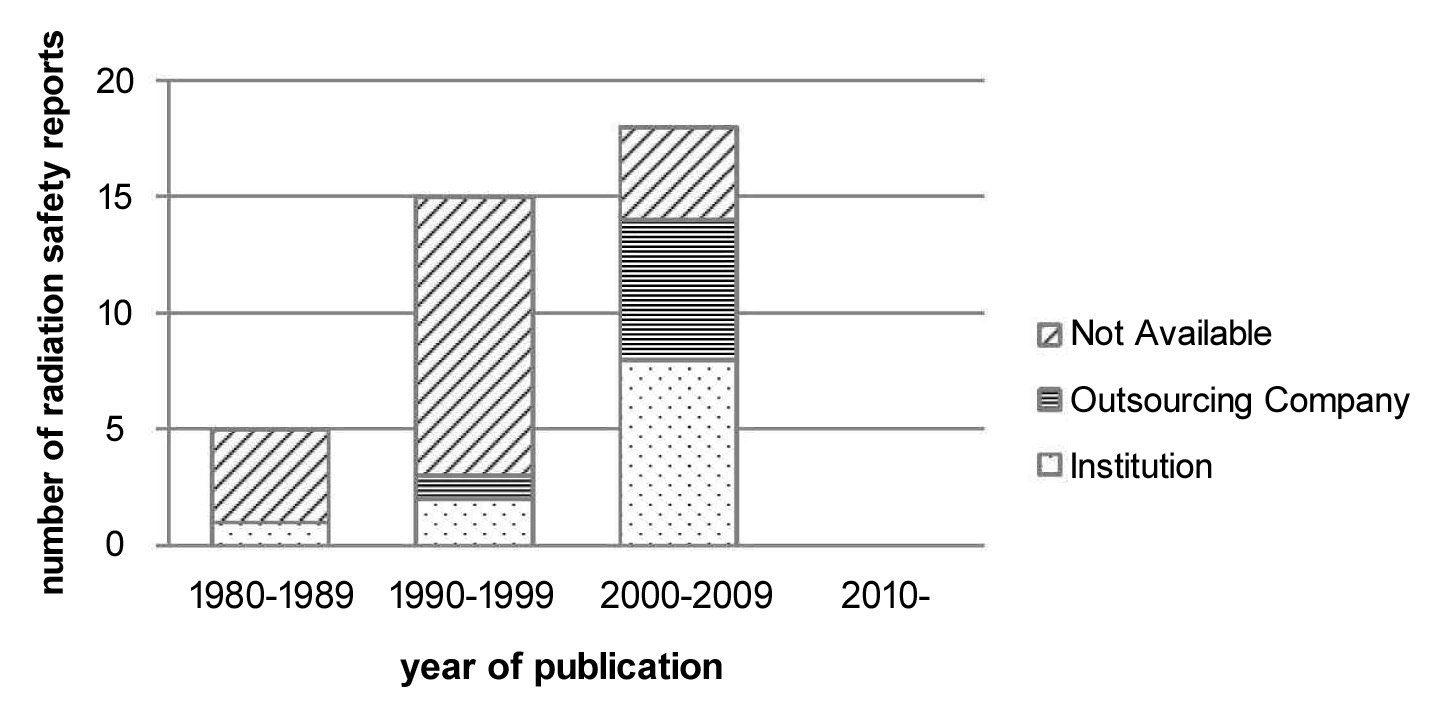
Since October 4, 2000, radiation safety control could be performed by an outsourcing company and thus caused the radiation safety documents that were completed by outsourcing agencies to increase in number. Indeed, the present study found that the radiation safety documents that were completed by outsourcing agencies rose from 6.7% in 1990-1999 to 33.3% in 2000-2009 (Fig.3). At present (2011), there are 13 outsourcing agencies that can complete radiation safety reports in Korea.6) However, despite the introduction of outsourcing agencies, the majority of the reports containing personal information of the drafter were still completed by institution-affiliated drafters: Figure 3 shows that in 1980-1989, 20.0% and 0.0% of the reports were completed by institution-affiliated personnel and outsourcing agencies, respectively. Similarly, in 1990- 1999, these values were 13.3% and 6.7%, respectively, and in 2000-2009, these values were 44.4% and 33.3%, respectively.
The Korean Nuclear Safety and Security Commission and American regulatory agencies such as the Nuclear Regulatory Commission (NRC) or NCRP require applicants to include radiation safety shielding calculations in their radiation safety reports.4) Report 151 of the NCRP defines
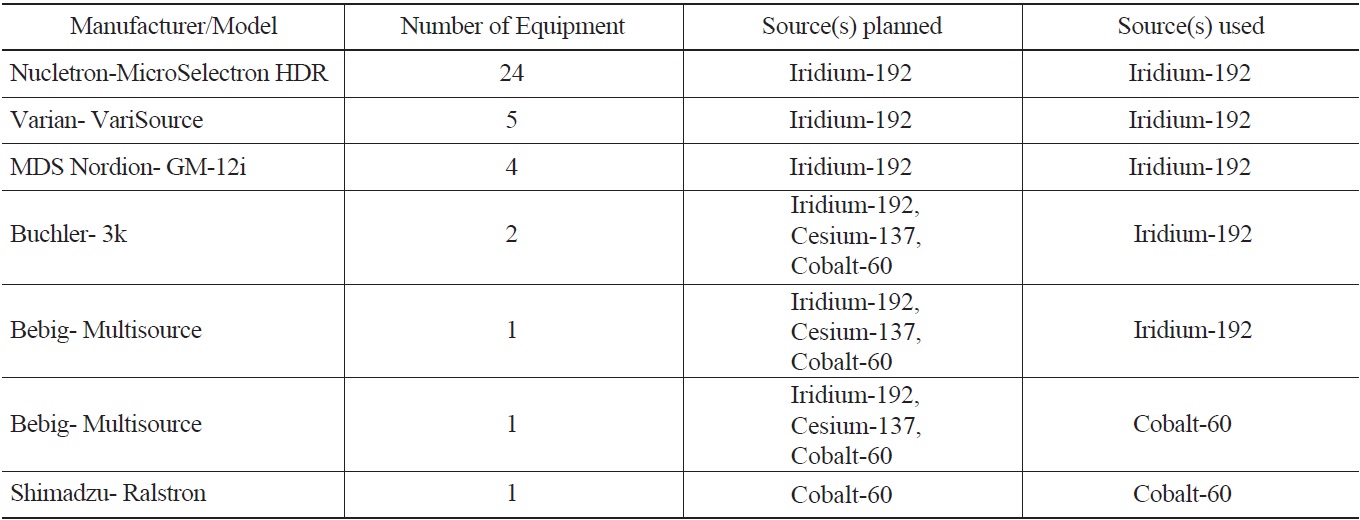
Number of Brachytherapy Units from Various Manufacturing Companies, Types of Sources when Brachytherapy Equipment Installation/Remodeling was Planned and Types of Sources that are Currently Being used in Korea
workload as ‘the average absorbed dose of radiation produced by a source over a specified time (most often one week) at a specific location’.4) Workload is a function of source activity and treatment time and is expressed by the following equation:

Γ (exposure rate constant) is exposure rate to activity at 1m;
f relates cGy to R;
A is the activity of the source;
t [treatment time (minutes) per week] is the time when the radioisotope is actually exposed in the air for treatment expressed in minutes per week.
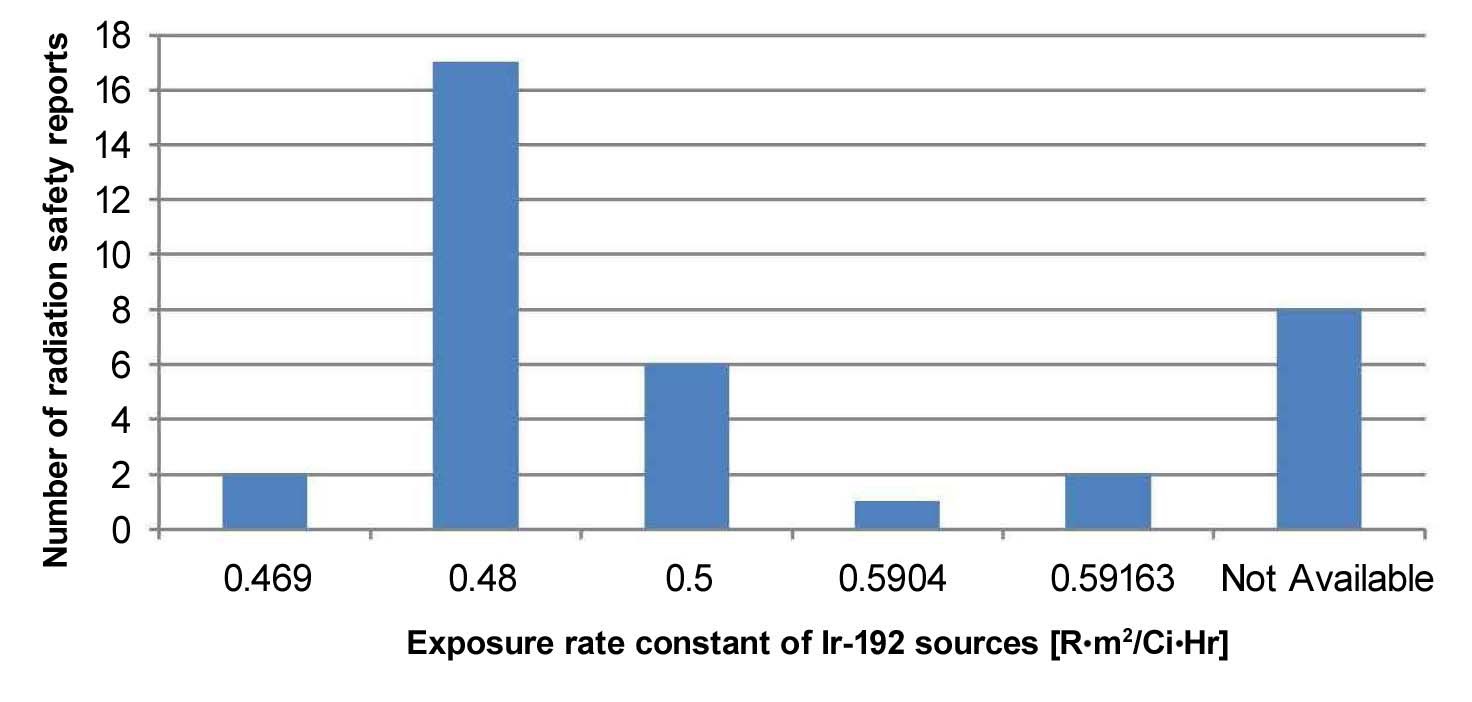
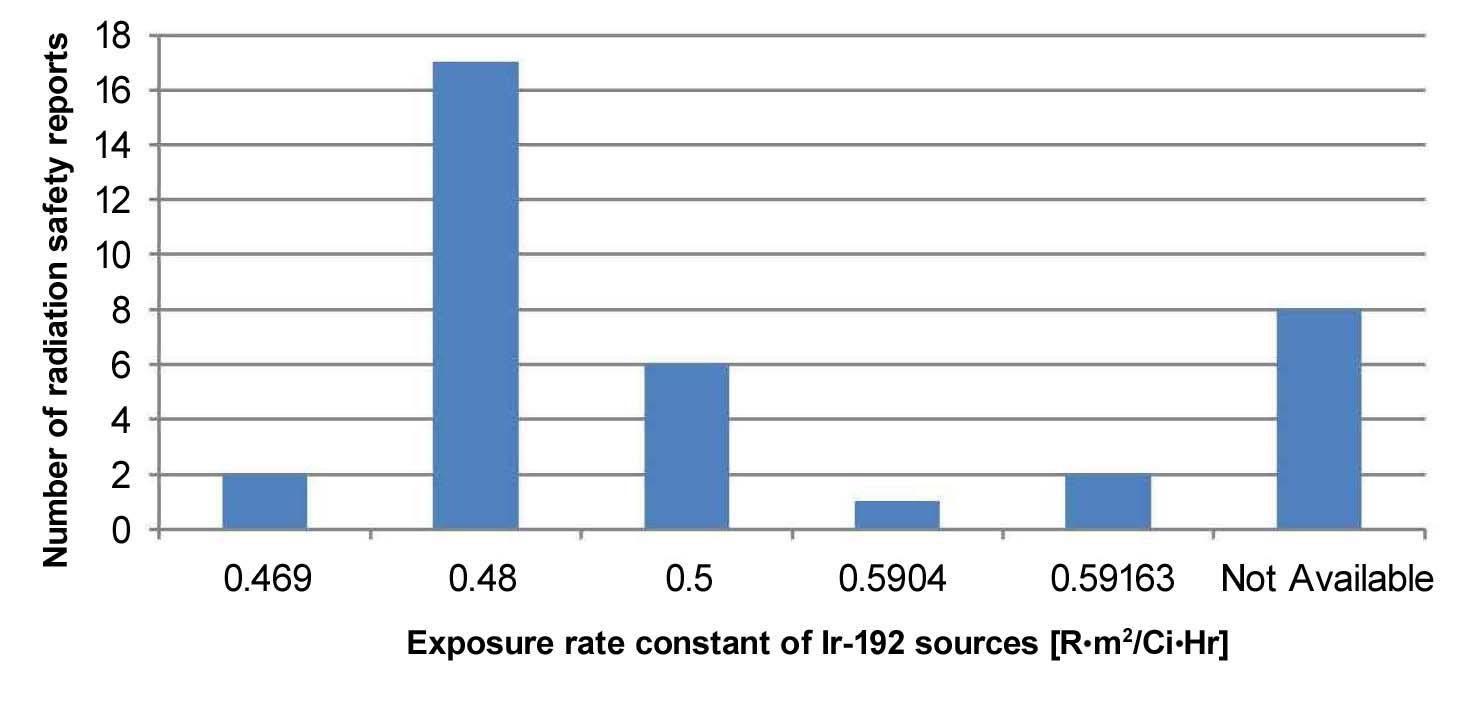
Different Γ, f, A, and t values from the various sources were used to calculate workload in the radiation safety reports. As shown in Figure 4, the exposure rate constant for Iridium-192 sources used to calculate workload ranged from 0.469 to 0.592 R·m2/Ci·hr, with 0.480 R·m2/Ci·hr being the most frequently used exposure rate constant (44.7%). Eight radiation safety reports (21.1%) failed to define the exposure rate constant. The exposure rate constant for
Cobalt-60 used in the radiation safety reports was either 1.2 or 1.32 R·m2/Ci·hr. Two of the five relevant radiation safety reports (40.0%) did not cite the exposure rate constant for the Cobalt-60 source.
Iridium-192 sources with an activity of 10Ci are used for HDR brachytherapy units. However, five of the radiation safety reports (13.2%) used Iridium activities of 11Ci, 12Ci or 13.6Ci to calculate the workload. This was the activity of the source at the time the equipment was installed or the shielding design goal was calculated. However, the actual treatment was carried out with an Iridium activity of 10Ci. Moreover, a radiation safety report from the radiation oncology department that performed the Bebig-MultiSource HDR treatment, which is capable of using three sources (Cobalt-60, Cesium-137 and Iridium-192), used Cobalt-60 with activity of 2Ci to calculate the workload. Currently, one department is using a Cobalt-60 source only, while another department is using an Iridium-192 source. In addition, a radiation safety report from the radiation oncology department that uses a Buchler-3k unit used sources of five different activities for workload calculation, including a Cobalt-60 with activity of 1.32Ci, Cesium-137 with activity of 2.04Ci and 2.08Ci, and Iridium-192 with activity of 8.35Ci and 6.74Ci. Through a personal interview, this department explained that at the time of brachytherapy equipment installation, five sources were used to treat gynecological cancer patients where a Cobalt-60 source was inserted into tandem and either two Cesium-137 or two Iridium-192 sources were inserted into ovoids to treat the site simultaneously. Currently, only Iridium-192 source with activity of 10Ci, which is supplied by a local company, is used for HDR treatment.
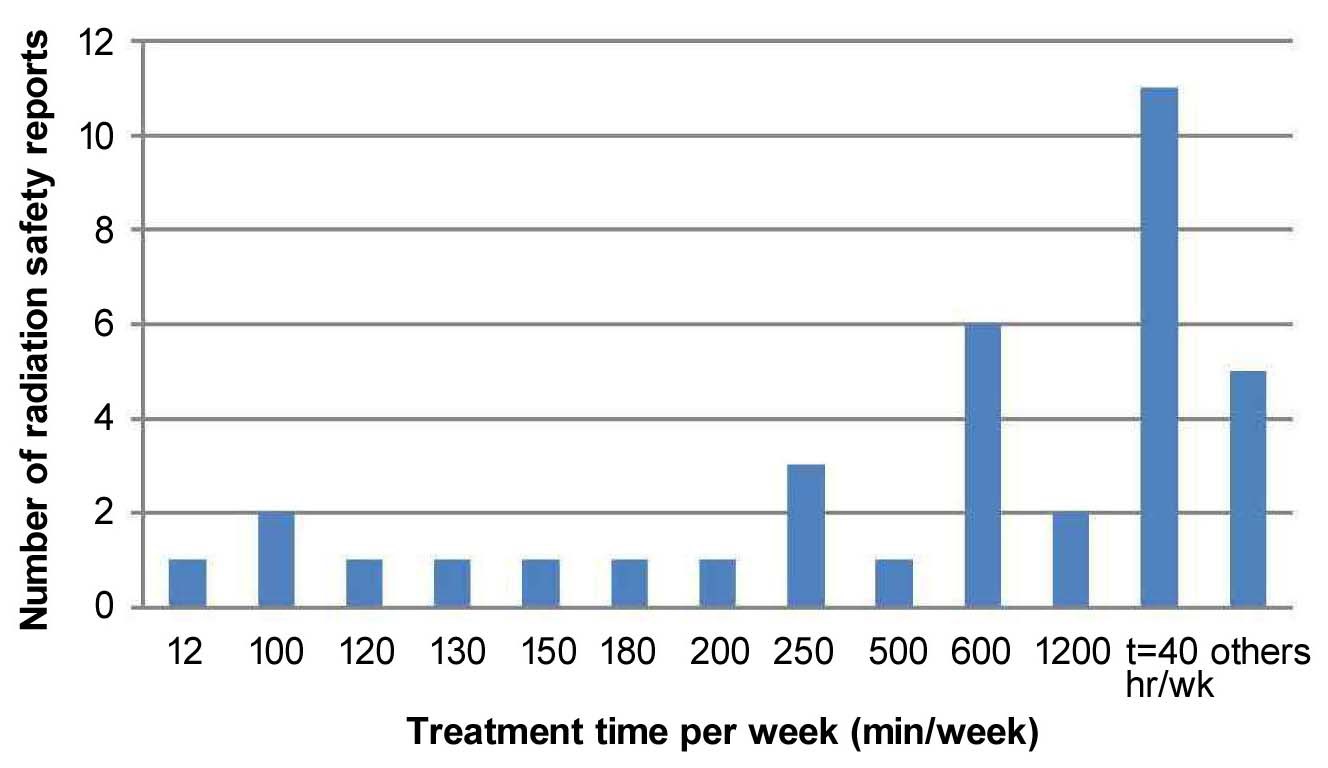
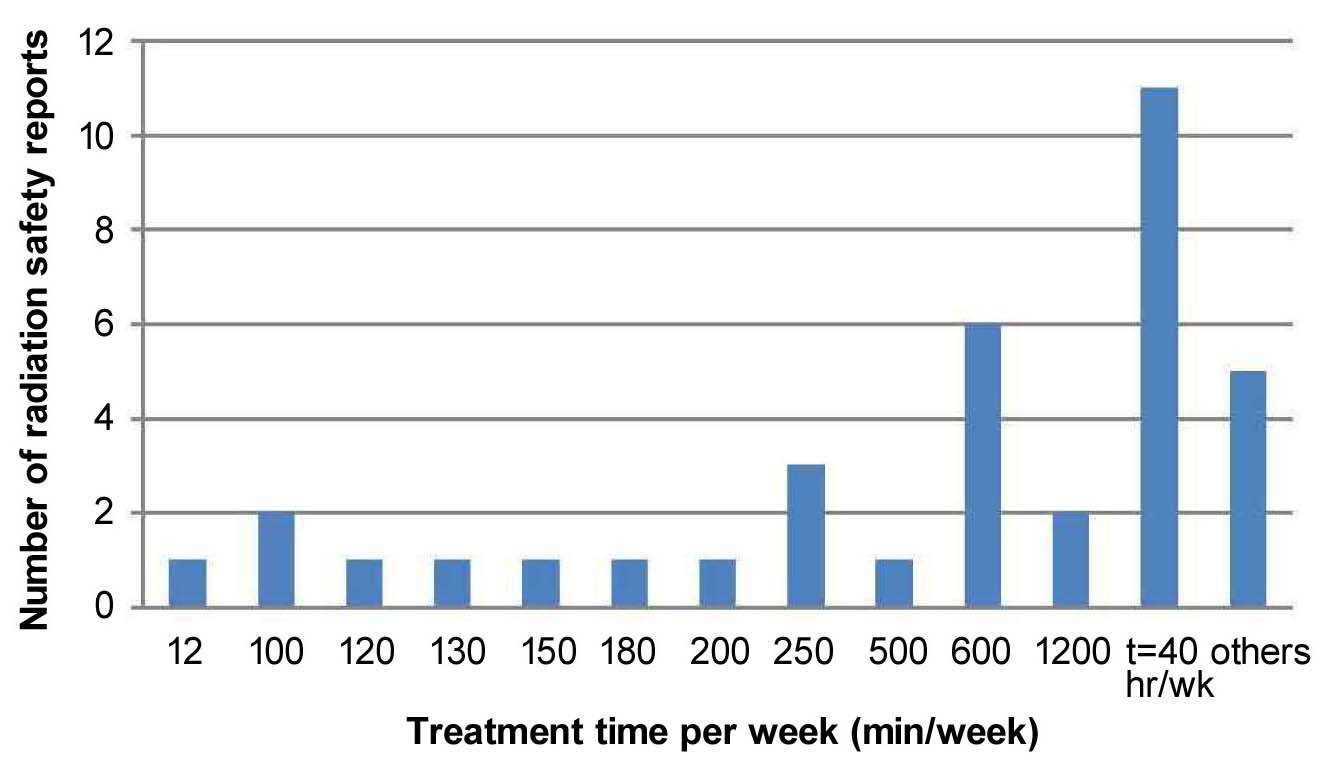
As shown in Figure 5, treatment time per week was not specifically defined in a large proportion of radiation safety reports (28.9%). These radiation safety reports assumed the time to be 40 hr/week (2,400 min/ week), which is used to calculate the workload for linear accelerators. However, a study by Glasgow and Dillman has shown that the average time estimate for 10Ci- Iridium-192 sources is 2 hr/wk (120 min/wk).7) Similarly, NCRP report 151 estimates the time for such
sources to be 6.7 hr/wk (402 min/wk).4) Thus, a treatment time assumption of 40 hr/week may be an overestimate. Of the radiation safety reports that actually calculated the treatment time, the most frequently used treatment time estimates used for calculating the workload were 100- 300 min/week (15.8%) and 600-700 min/week (15.8%).
Various recommended shielding design goal values were used in the radiation safety reports. The most frequently used shielding design goal value for a controlled area was 1 mSv/week (21.1%), followed by 0.3 mSv/week, which is equivalent to 50 mSv/year (10.5%). The most frequently used shielding design goal value for an uncontrolled area was 0.1 mSv/week (23.7%), followed by 0.02 mSv/week (15.8%). Four reports (10.5%) used an instantaneous dose rate (IDR) of 2.5 mR/hr for controlled areas and 0.25 mR/hr for uncontrolled areas.
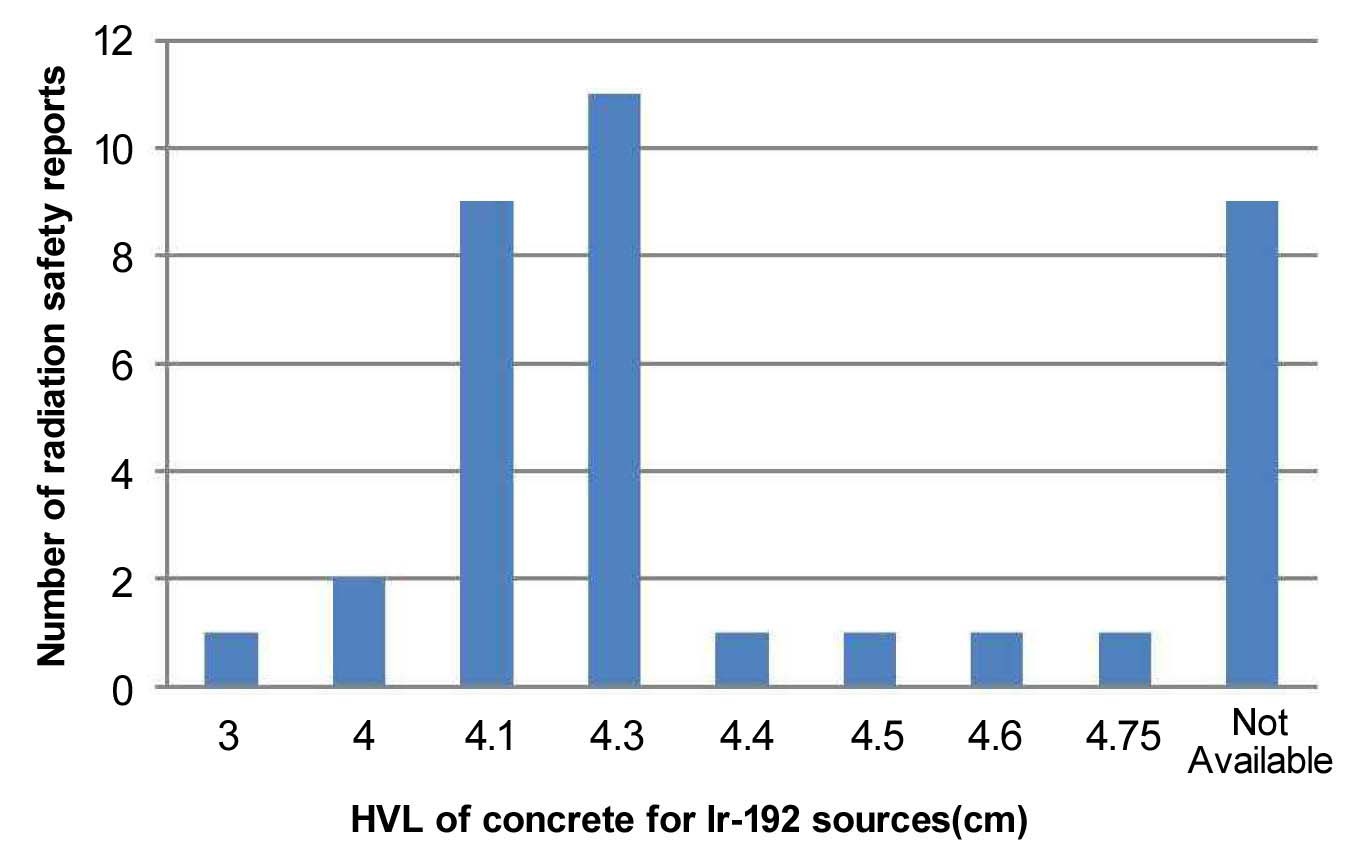
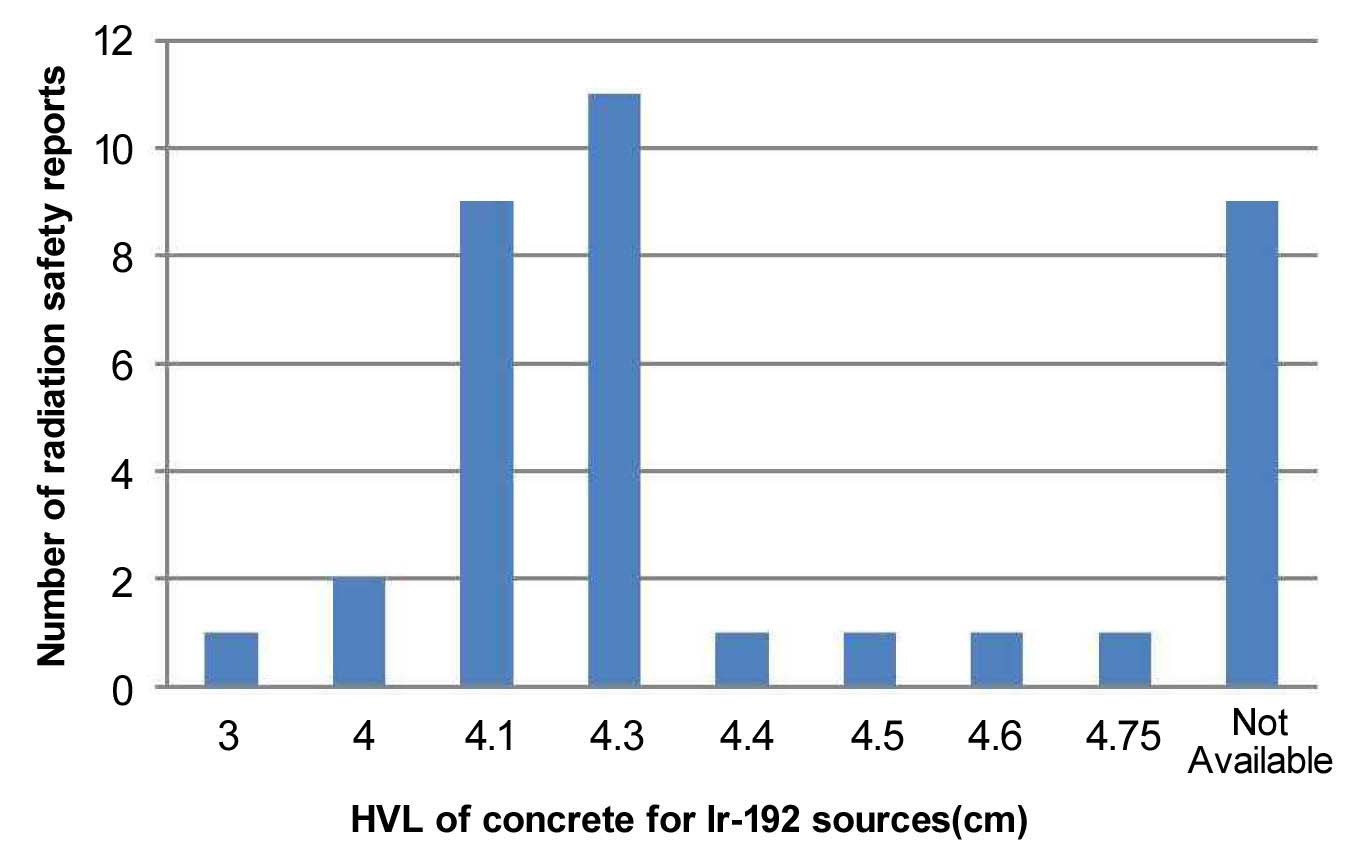
As shown in Figure 6, the HVL of concrete for Iridium- 192 ranged between 3 and 4.75 cm. The most frequently used HVL values for Iridium-192 were 4.1cm(23.7%) and 4.3 cm (28.9%) suggested by NCRP Report 49.3) The HVL of 3 cm was obtained by the equation:

where μconc = 0.23/cm.
The HVL values of 4.0 cm, 4.5 cm and 4.55 cm were obtained by calculations using transmission factor (B value) and the equation:

Substituting μ from equation (2) into equation (3) yields:

Nine radiation safety reports (23.7%) did not include concrete HVL values for Iridium-192.
The HVLs of steel used in the shielding calculation were 0.9 and 1.3 cm. Most radiation safety reports (65.8%) either did not use steel for facility shielding or did not include this HVL for the shielding calculation.
The HVLs of lead used in the shielding calculations ranged between 0.2 cm and 0.6 cm. The HVL of 0.6 cm that is suggested by NCRP Report 49 was the most frequently used HVL value for Iridium-192 (47.3%).3) Thirteen radiation safety reports (34.2%) either did not use lead for facility shielding or did not include HVL for shielding calculations.
TVL mentioned here are first tenth-value layers (TVL1) and equilibrium tenth-value layers (TVLe) have not been assessed since most radiation safety reports did not consider the spectral changes of radiation emitted from Ir-192 sources.
This study evaluated the quality of radiation safety reports of the current brachytherapy units in Korea, which were installed between 1985 and 2010. The majority of the brachytherapy units in the radiation oncology departments in Korea were supplied by Nucletron (63,2%), followed by Varian (13.2%) and MDS Nordion (10.5%). All 38 radiation oncology departments treated their patients with the HDR brachytherapy technique. However, four departments had brachytherapy units that could treat patients with both LDR and HDR techniques
National as well as international guidelines stipulate that radiation safety reports should contain the personal information of the drafter. A significant number of the reports (47.4%) included this information. Moreover, 28.9% of the reports were completed by radiation oncology department-affiliated people while 18.4% were completed by outsourcing companies; the remaining reports did not provide drafter information.
Factors used for shielding calculations, namely exposure rate constant and HVL value, showed acceptable variation. The exposure rate constant values for Iridium-192 sources used in workload calculation varied acceptably between 0.469 and 0.592 R·m2/Ci·hr. The HVLs of concrete, steel and lead for the Iridium-192 sources that were used for shielding calculation did not vary significantly.
However, the treatment time per week, which was used to calculate workload, varied widely (ranging from 12 to 2,400 min/week). The treatment time approximation that was most frequently employed (28.9% of all reports used this) was 40 hr/week, which is a typical treatment time for linear accelerators. Due to the limitations of this study, the estimated treatment time used for calculating workload could not be compared to the actual treatment time. Therefore, we cannot conclude whether treatment times of 12 or 2400 min/week were actually used in the clinic, or whether these estimations are incorrect. However given the average treatment time estimations that were suggested by Glasgow and Dillman (120 min/week) and NCRP Report 151 (402 min/week), a treatment time of 2,400 min/week seems likely to be an overstatement 4, 7).
The evaluated TVLs are first tenth-value layers (TVL1) and equilibrium tenth-value layers (TVLe) have not been assessed since most radiation safety reports did not consider the spectral changes of Ir-192 sources possibly due to the low energy of radiation emitted.
The installation of brachytherapy units has been decreasing since 2001. Nevertheless, it is still necessary to ensure appropriate and safe radiation facility shielding. Moreover, it can be expected that older brachytherapy machines will eventually have to be replaced with new units. It should also be remembered that given the current preference for brachytherapy treatment with HDR techniques, even minor mistakes could result in significant consequences. While such accidents are believed to be generally under-reported, ICRP Publication 97 states that over 500 HDR events have been recorded.8) One of the most severe incidents involved a patient receiving interstitial HDR treatment for anorectal cancer. An error occurred while the source was being inserted in the catheter and it went unnoticed that the source was left in the body. The patient died five days later as a result of this grave error.8)
One potential problem is that with the introduction of outsourcing agencies, more centers are relying on these agencies for completing radiation safety reports. While these agencies are well-trained and possess expert knowledge in the completion of radiation safety reports, they are not aware of the actual clinical environment and the status of technical advancements in the radiation oncology field. Although, the development of brachytherapy technique is not as rapid as that of EBRT it cannot be ensured that the possible changes have been reflected accurately in the radiation safety reports. Moreover, persons completing radiation safety reports who are affiliated with the institutions may not possess expert knowledge in radiation protection and shielding, since they are mainly medical physicists and not radiation safety officers. Thus, more practical guidelines should be in place for drafters to reference from, when completing the radiation safety reports. The results of the present study may aid the development of such guidelines for completing radiation safety reports for brachytherapy equipment in radiation oncology departments in Korea.
The present study revealed that although the majority of radiation oncology institutions showed good agreement in terms of completing radiation safety reports, a few of the reports varied in estimations of the treatment time, which in turn led to variations in the estimations of workload. The need to ensure safety when operating brachytherapy equipment, the fact that new brachytherapy units are likely to be installed in the future, and the fact that outsourcing agencies are increasingly being used to complete radiation safety reports means that standard guidelines that more realistically reflect the current clinical situation of radiation oncology departments in Korea are needed.