The glossopharyngeal nerve (CN IX) and the vagus nerve (CN V) are involved in taste, speech impediments, and swallowing and are often damaged together because they exit side by side at the brain stem (upper medulla), and have similar and overlapping anatomical and functional distributions in the periphery. Damage to CN IX & V results in loss of bitter and sour taste and impaired swallowing [1,2]. The hypoglossal nerve (CN XII), which originates from the hypoglossal nucleus near the midline in the dorsal aspect of the medulla, innervates the muscles of the tongue and is related to the control of voluntary movement of the tongue [1,2].
With damage of CN XII, the tongue has weakness, atrophy, fasciculations on the side of the involvement, and a deviation toward the affected side when the tongue is stuck out. The causes of twelfth-nerve palsy have been reported to be tumors (the first most common), trauma [3,4] (the second most common), strokes, hysteria, multiple sclerosis, surgery, autoimmune disease, Guillain-Barre’ neuropathy, internal carotid artery dissection [5], extracranial internal carotid artery aneurysms [6], idiopathy [7], and infections [8,9].
Hypoglossal nerve palsy is a rare disease, but has several cases of this disease have been reported [8-10]. On the other hand, CN IX & X palsy has very few reports except for cases caused by upper respiratory infection [11]. The cause of CN X & XII palsy, which was similar to the symptoms of our case, was internal carotid artery dissection [12].
Few reports on the cases of idiopathic CN IX, X, and XII palsy treated with Korean traditional treatment exist. Thus, this study reports a rare case in which a combination treatment of acupuncture, pharmacopuncture, and herbal medicine had an effect on a male patient with ninth, tenth, and twelfth cranial nerve palsy of unknown origin.
2.1. Characteristics of patient and medical history
A 39-year-old man visited our Korean Internal Medicine Department complaining of a severe headache over his left parietal region, left-sided tongue weakness, loss of taste and sensation on the left side of his inside tongue, a slight alteration in speech, vague swallowing difficulty, and indigestion for 5 days. There was no past history except Bell's palsy one year earlier and gastritis six months before. The medical history showed no trauma, other illnesses,
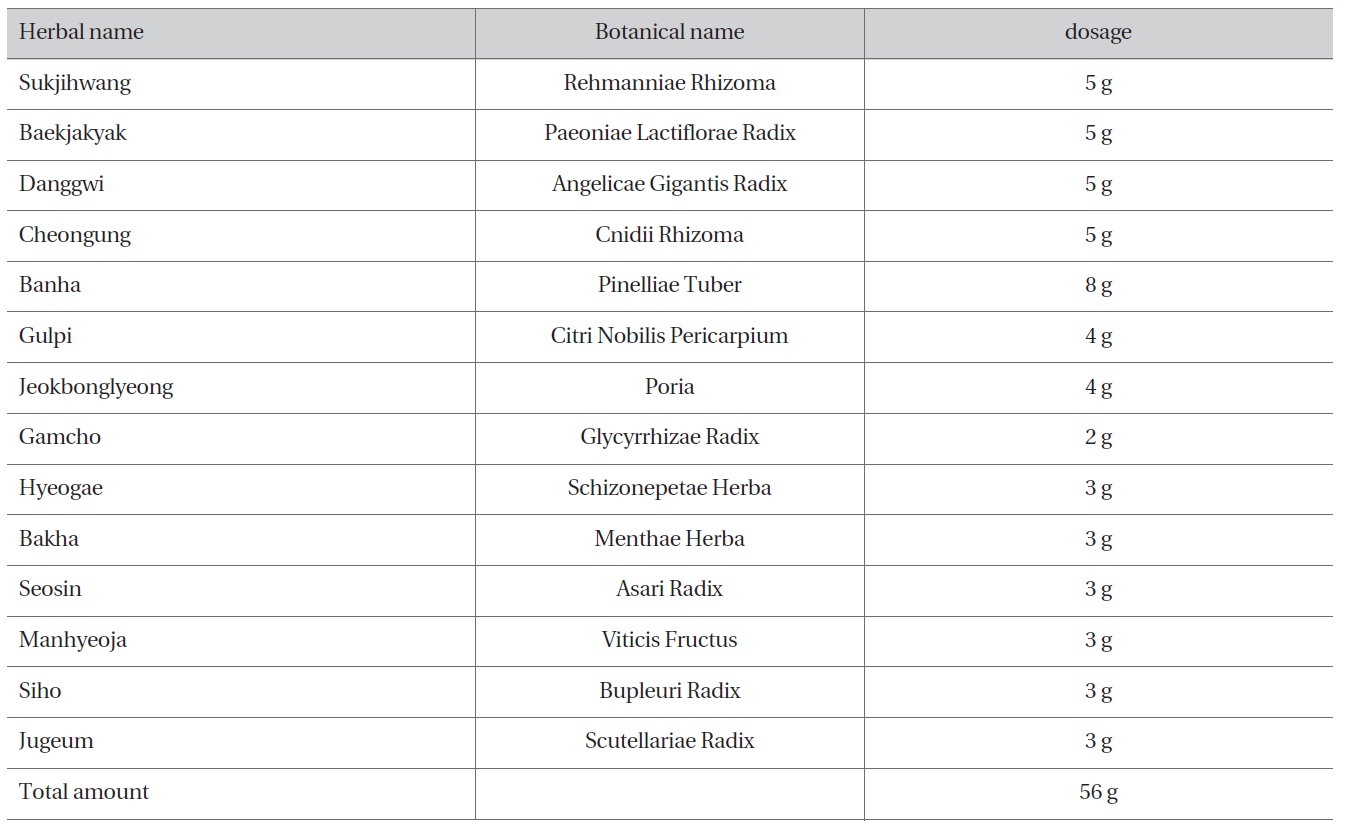
[Table 1] The Prescription of zhuapiandutongbang
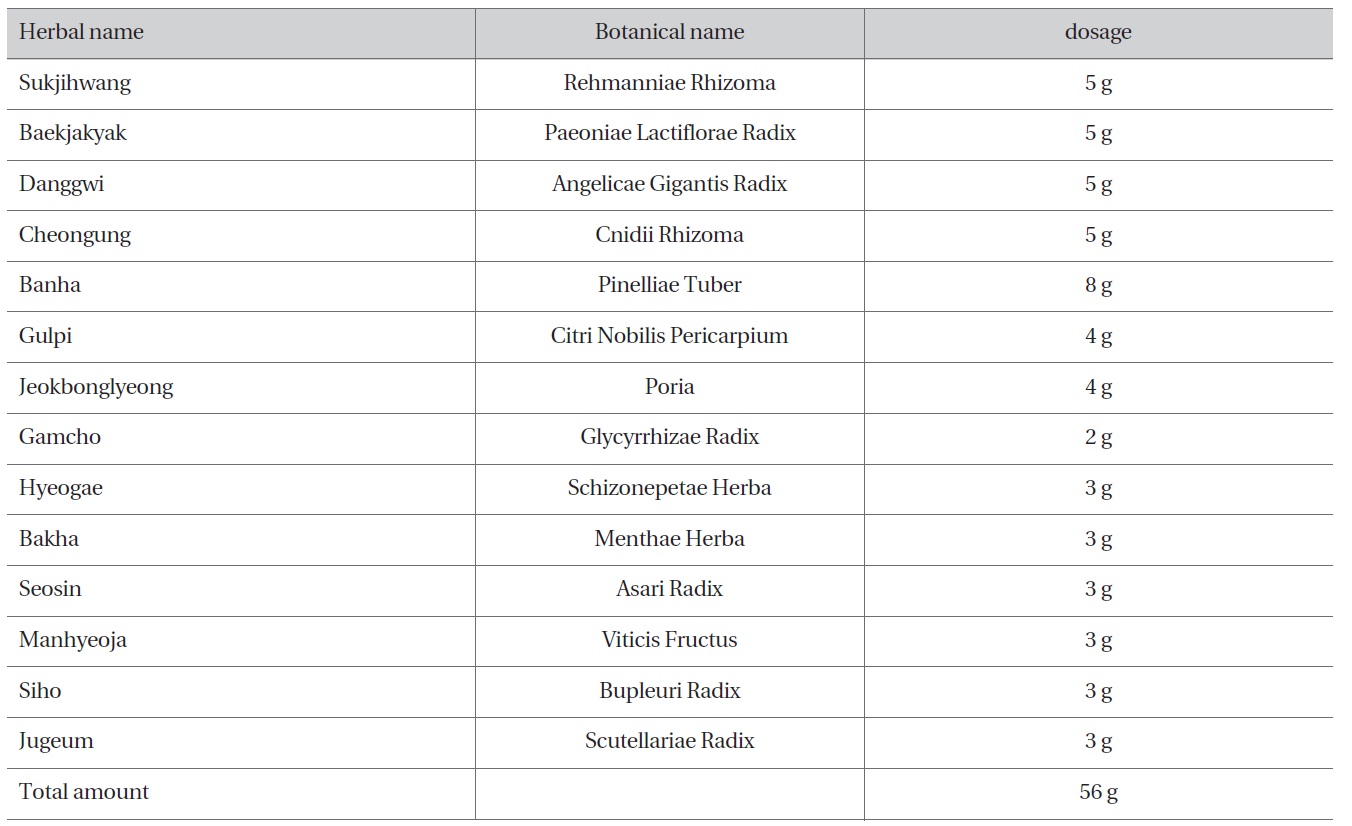
The Prescription of zhuapiandutongbang
family history of disease, medications, smoking, drinking, and so on. He had not caught a common cold, nor had be received any vaccination or specific treatment before his first visit.
On neurological examination, his tongue deviated to the left on protrusion but no atrophy or fasciculations were observed. Mild right-sided deviation of the uvula and a decreased gag reflex on the left side of the throat were observed. The other pathological reflexes were normal. Magnetic resonance imaging (MRI), with and without gadolinium, and computed tomography (CT), with and without enhancement, of the brain, brain stem, upper neck, and skull base were normal. Laboratory tests and electrocardiography were also normal. The syndrome differentiation of the patient was categorized as the syndrome of ascendant hyperactivity of liver yang with heart fire on the grounds that overwork and much stress had given a rise to a flushed face, bitter taste, thin dry tongue coating in the mouth, palpitation, and string-like pulse
2.2.1. Pharmacopuncture
From among the types of eight principle pharmacopuncture (EPP) a 0.2-mL dosage of Hwangyeonhaedoktang pharmacopuncture was administered at CV23 and CV17, respectively, at a perpendicular angle and a 0.5-mm depth
by using the tapping method [13].
2.2.2. Acupuncture
0.25 mm × 3.0 mm stainless needles (Dongbang Acupuncture Inc., Korea), was applied at P06, Li05, TE05, and G37 on the right side of the body at depths of 0.5~1 cm, a total of 4 needles, by using neutral supplementation and draining (平補平瀉) for 20 minutes.
2.2.3. Herb medicine
Zhuapiandutongbang(左偏頭通方)was administered at 30 minutes to 1 hour after mealtime three times a day for 5 days. Herbal compounds, a twentyfold dosage of the total
amount in Table 1, were decocted in 6000 mL of water for two to three hours. The extracted liquid was packed in 15 pouches, 120 mL per pack. The composition of zhuapiandutongbang is shown in Table 1.
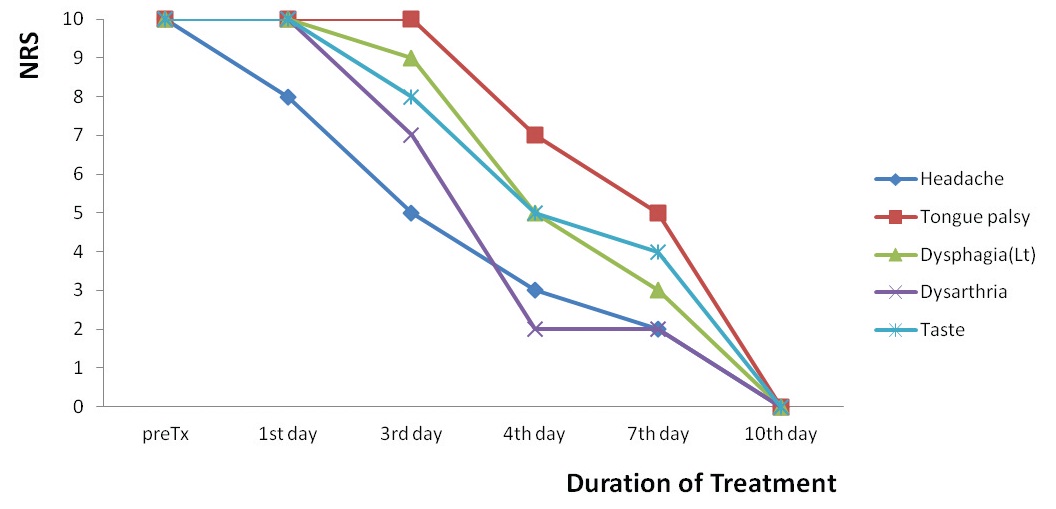
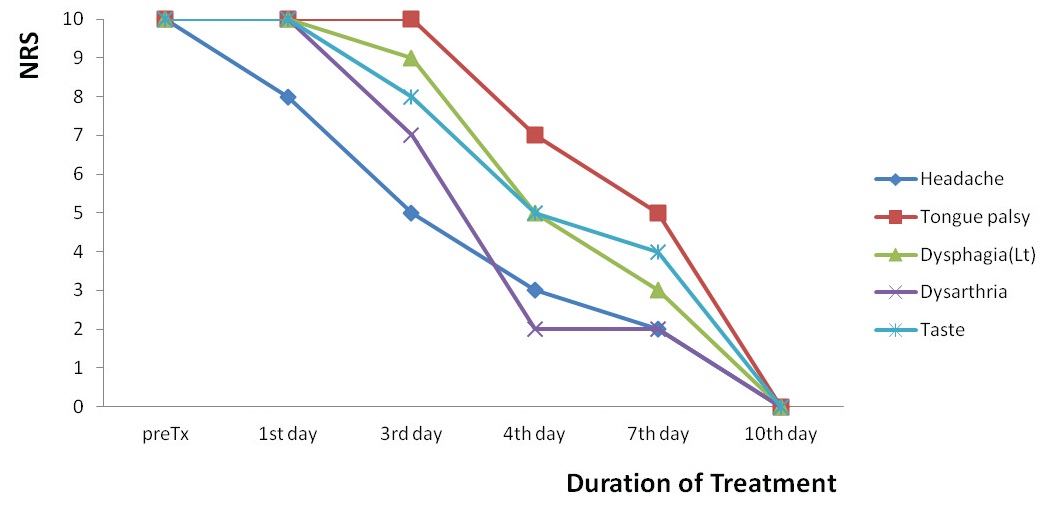
2.3. Progress of symptoms (
The severity of headache was decreased 20% on the first day of treatment, 50% on the third day, 70% on the 4th day, and 100% on the 10th day. Herbal medicine was stopped on the 6th day of treatment because of cost problems. The left-sided deviation and the weakness of tongue were improved 30% on the 4th day and 100% on the 10 days of treatment (Figs. 1-3). The swallowing difficulty was
recovered 10% on the 3rd day, 50% on the 4th day, and 100% on the 10th day of treatment. The mild dysarthria on the left side of throat was restored 30% on the 3rd day, 80% on the 4th day, and 100% on the 10th day of treatment. The taste and the sensation of the tongue were regained 20% on the 3rd day, 50% on the 4th day, and 100% on the 10th day of treatment.
Mild dysarthria on the left side of the throat and loss of taste and sensation on the left side of the inside tongue were caused by CN IX and X palsy, and the left-sided deviation of the tongue on protrusion and tongue weakness were caused by CN XII palsy. CN IX and X are more often damaged together because of their anatomical and functional similarity [1]. The cause of CN IX, X and XII palsy couldn't be identified despite the detailed medical history and all the studies, such as brain MRI, brain CT, and other examinations, so that this disease was diagnosed as idiopathic CN IX, X and XII palsy [10]. Acupoints CV23 to treat tongue palsy and CV17 to relieve heart fire and liver yang were selected with Hwangyeonhaedoktang pharmacopuncture among the types of EPP [13]. P06, the pericardium meridian's connecting point; Li05, the liver meridian's connecting point; TE05, the triple energizer meridian's connecting point; and GB37, the gallbladder meridian's connecting point were used for acupuncture after pharmacopuncture treatment. The left parietal region in the head is the course of the gallbladder meridian, and the same lesser yang meridian is the triple energizer meridian. The lesser yang exterior-interior meridian is the pericardium meridian and the liver meridian. The liver's five body constituents are tendons. The liver meridian was selected to treat dysphagia and the tongue's palsy and weakness. The gallbladder meridian and the liver meridian have an exterior-interior relationship. The connecting point of both the reverting yin meridian and the lesser yang meridian was selected because the connecting point could connect and enforce the exterior-interior relationship of the twelve meridians closely [14,15].
Zhuapiandutongbang, ≪Dongyibogam(東醫?鑑)≫[16], is a prescription that combines Samultang (四物湯) with Leejintang (二陳湯), to which Schizonepetae Herba 3 g, Menthae Herba 3 g, Asari Radix 3 g, Viticis Fructus 3 g, Bupleuri Radix 3 g, and Scutellariae Radix 3 g are added. Based on literature [16,17], it was used to relieve left-sided headache. This herbal medicine was administrated for 5 days at first, and the severity of headache was markedly decreased although the medication was halted due to the cost. The acupuncture and pharmacopuncture treatment, however, continued until the symptoms disappeared on the 10th day.
Several reports on CN XII palsy with ipsilateral headache [18], CN IX and XII palsy [6], unilateral CN XII palsy [10], and CN X and CN XII palsy [12] exist in the literature. The causes of these diseases are diverse, such as internal carotid artery dissection, trauma, external and internal carotid artery aneurysms, idiopathy and so on. This case, in which CN IX & X palsy and CN XII palsy with severe ipsilateral headache occur together and are idiopathic, is thought to be a rare condition. In addition, no reports of Korean medicine treatment for CN IX, X and XII palsy seem to have been published to date even though many reports on different cranial nerve palsies, such as oculomotor nerve palsy [19], and facial nerve palsy [20,21], do exist.
Isolated idiopathic CN XII palsy cases similar to my case have been reported to have been treated with dexamethasone and prednisolone in Western medicine. However, the treatment duration of my case was shorter than that of the Western medicine treatment [22].
This study has limitations. Which of the three types of treatments were more effective could not be identified, and the results cannot be generalized based on one case report. Nevertheless, the results suggest that the rare and idiopathic CN IX, X, and XII palsy of unknown origin may be effectively treated by using Korean medicine.
Korean medicine treatment such as acupuncture, pharmacopuncture, and herbal medicine is suggested to be effective in treating idiopathic ninth, tenth, and twelfth cranial nerve palsy with ipsilateral headache.