According to the Korea national data on deaths in 2010, 73,145 patients died of cancer, and cancer was the leading cause of death [1]. Over the past 10 years, the figures have been growing each year [2]. According to the Korea national data in 2010, each year over 200,000 people were diagnosed with cancer, with a total of around 400,000 cancer patients [2]. Most cancer patients considered receiving conventional (Western) treatments, such as surgery, radiation therapy, and immune therapy. However, the treatment rate for patients in the terminal stage of cancer was low, and they were more likely to have side effects and to psychologically reject cancer therapy; these patients were more likely to seek complementary and alternative medicine (CAM) therapies or traditional medicine. The booming well-being environment even caused many people to turn their eyes to CAM [3, 4]. Most cancer patients receive a combination of CAM and Western medicine treatment. According to national research, 75% of patients who undergo Western cancer treatments are reported to have used CAM. Cancer patients also spend 2,020,000 KRW (1,808 USD), on average, for treatment, and that cost constitutes 31.1% of medical payments, on average [1].
Nowadays, interest in well-being and holistic lifestyles has increased the interest in CAM, which seeks to improve the quality of life in a broad context [5, 6]. CAM includes vitamin therapy, diet therapy, diet method, massage, acupuncture, aromatherapy, yoga, music therapy, and meditation, all of which are methods that can modulate the body and the mind [7, 8]. Diet and nutrition therapy are the most commonly used therapies when treating cancer with CAM. In relation to nutrition therapy, the consumption of health supplements is growing year by year because patients with cancer and other disease, as well as healthy people, are interested in health supplements.
Information on CAM can be obtained through the internet and many books. However, especially for CAM, its content and standards are not clear, so the available information is diverse. Under the current law, control of false advertising and protection of consumers are limited by legal constraints. The medical system changed in 2010 to allow Western medicine departments (or clinics) to be established in Oriental medicine hospitals and vice versa, but Western medical doctors cannot prescribe Oriental medicines and Oriental medical doctors cannot use diagnose or treat patients using Western devices, so the interaction between the two medical groups is very weak.
Many factors are involved in choosing the method for treating and/or preventing disease. Therefore, the importance of CAM management should be stressed for many reasons. Also, from now on, whenever the government considers the management and quality control of providers of CAM or Oriental medicine to patients with cancer, it should elicit background data.
Based on international and national data concerning the providers of CAM, the management of CAM and the utilization status of CAM for treating cancer patients, our team designed a questionnaire named the “Survey on the Supply Pattern of Complementary and Alternative Medicine for Cancer Patients” Also, we consulted with CAM experts who participated in our workshop; then, we finished making the questionnaire through a pilot survey given to a few CAM providers in January 2008.
The questionnaire consisted of 38 questions. The surveyees needed to answer some questions by setting priorities such as 1st, 2nd and 3rd. The questionnaire contained 5 sections: CAM procedure for treating cancer patients (17 questions), standard operational protocol (or procedure) and disputes/administrative dispositions during CAM therapy (4 questions), qualification of CAM providers (5 questions), management methods to control CAM (4 questions), and general characteristics of the surveyees (8 questions).
We searched the on-line homepage manager concerning CAM in cases when the e-mail address or address could be obtained, professors or staff members who teach CAM at institutes or schools, students who graduated from or were currently enrolled in CAM related departments in 2008, medical doctors or Oriental medical doctors conducting procedures of CAM on cancer patients, and members of CAM related academic societies. About 350 surveyees were selected. When the e-mail address could be obtained, we sent questionnaires and an explanation three times in February 2008. We visited educational institutes or schools or sent postal mail to them during March and April 2008. In spring seminars of CAM related academic societies, a member of our team visited the seminar, explained the survey and gave instructions on how to complete the questionnaire. To improve the completion rate, we used a few gift incentives, like an USB.
The number of collected questionnaires was 182 papers (completion rate: 52.0%). After examining all the questionnaires collected and excluding some because they lacked data, we were left with 168 papers. The 168 surveyees included Oriental medical doctors, doctors and nurses as medical professionals, acupuncturists, clinical art therapists, alternative therapists, chiropractors, trainees of traditional Chinese medicine, feet massage therapists, laughter therapists, Qi gong therapists. We classified them into two groups, medical professionals and other CAM providers, and we analyzed the data for those two groups. The number of medical professionals was 19 (11.3%), and the number of other CAM providers was 65 (38.7%); other, including those with missing data, numbered 84 (50.0%). All statistical analyses, such as frequency analyses, chisquared tests, and analysis of variance (ANOVA), were performed using SPSS 12.0 for Windows®.
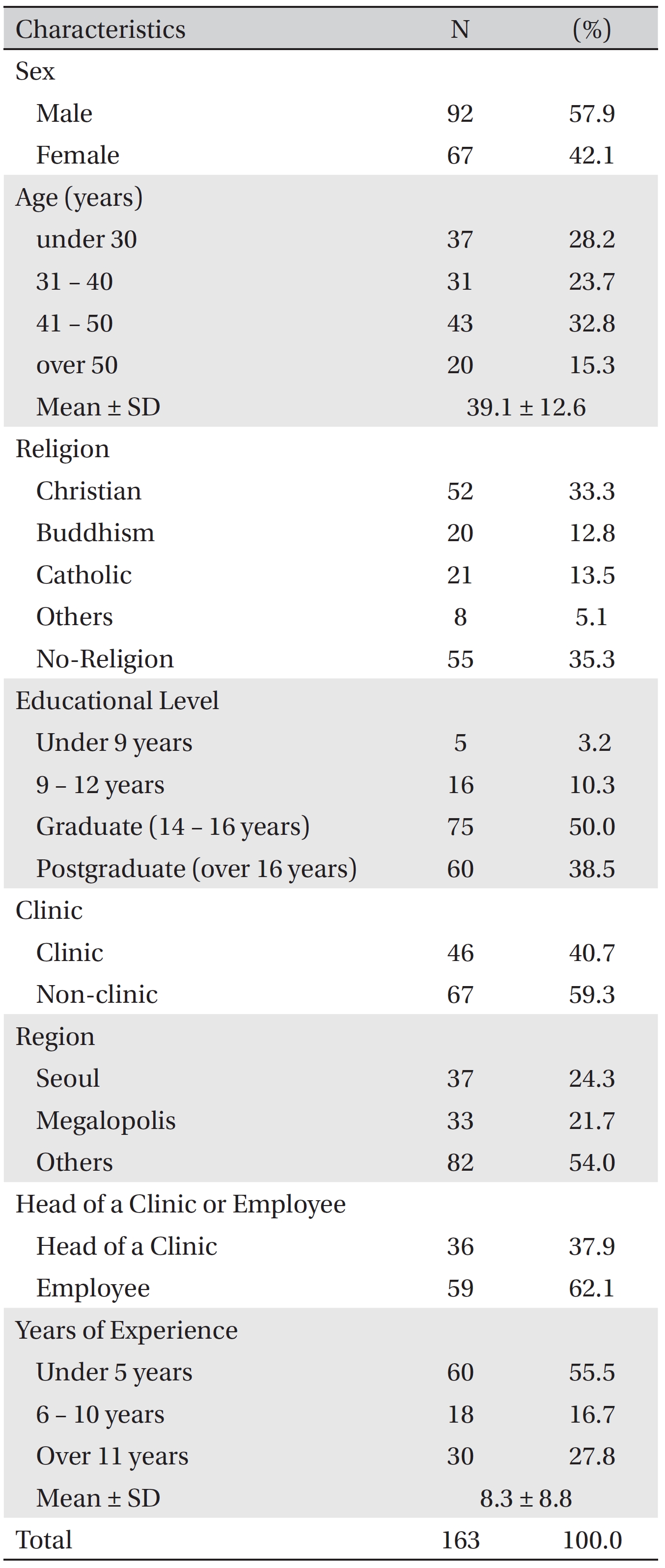
There were not significant differences according to sex and age. As the religious affiliation of the surveyees, most identified with no religion (35.5%) or Christian (33.3%). Most surveyees had a graduate or postgraduate education (88.5%). Of the surveyees, 55.5% had careers of less than 5 years, and 27.8% had careers of more than 11 years (Table 1).
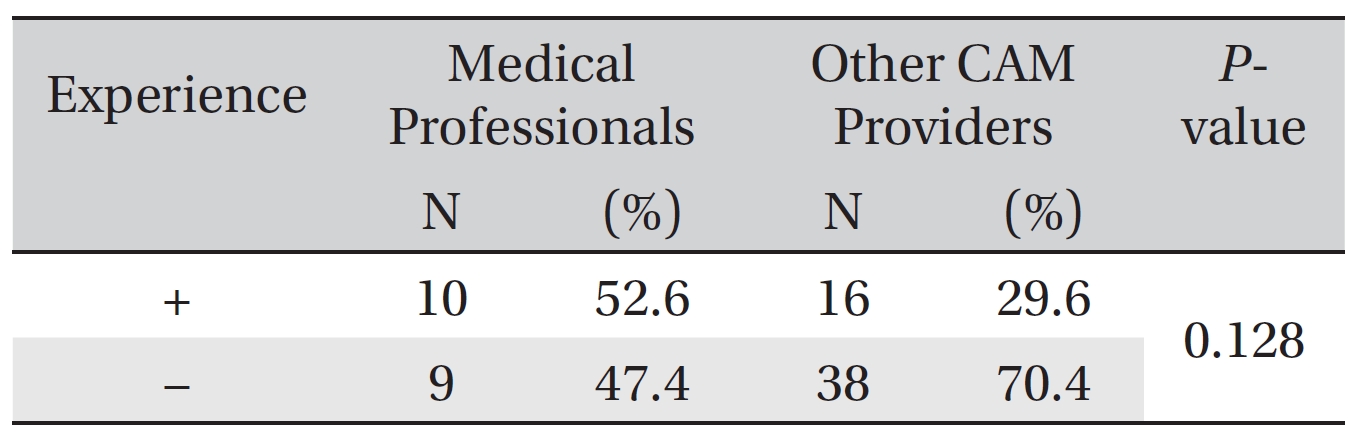
Overall, concerning the question about experience with providing CAM to treat cancer patients, 35.6% of the surveyees responded that they had had such experience. In detail, 52.6% of the medical professionals responded that they had had such experience, as did 29.6% of the other CAM providers (
[Table. 1] Socioeconomic characteristics of the surveyees
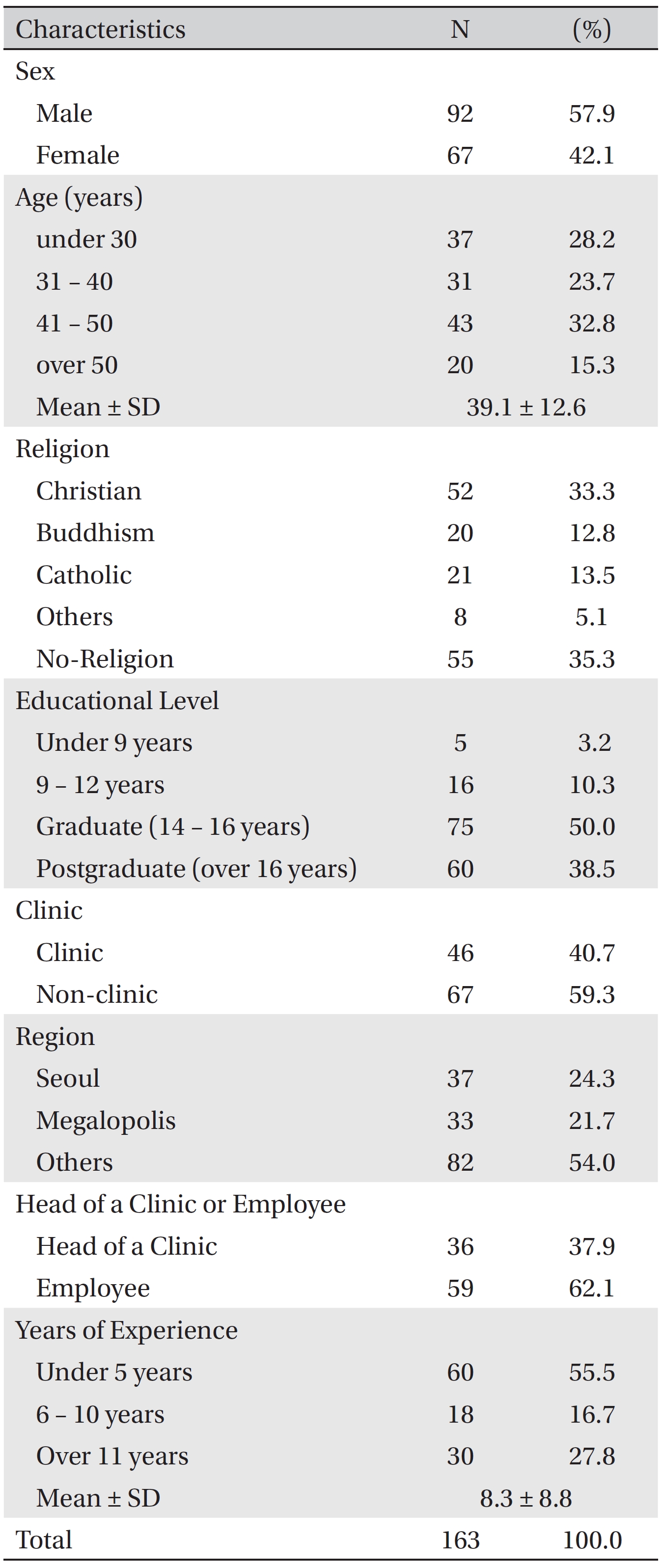
Socioeconomic characteristics of the surveyees
[Table. 2] Experience with CAM procedures for cancer patients
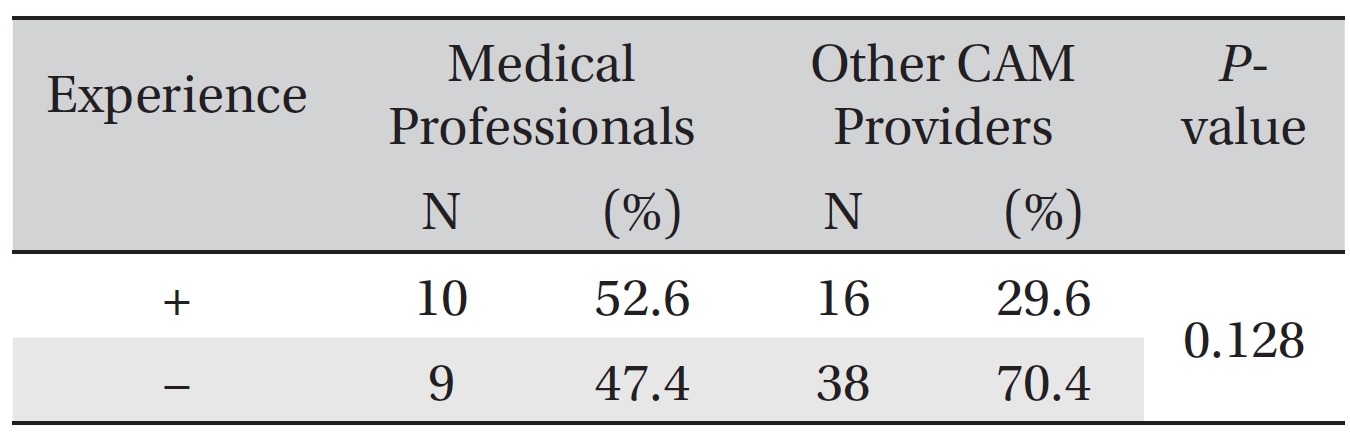
Experience with CAM procedures for cancer patients
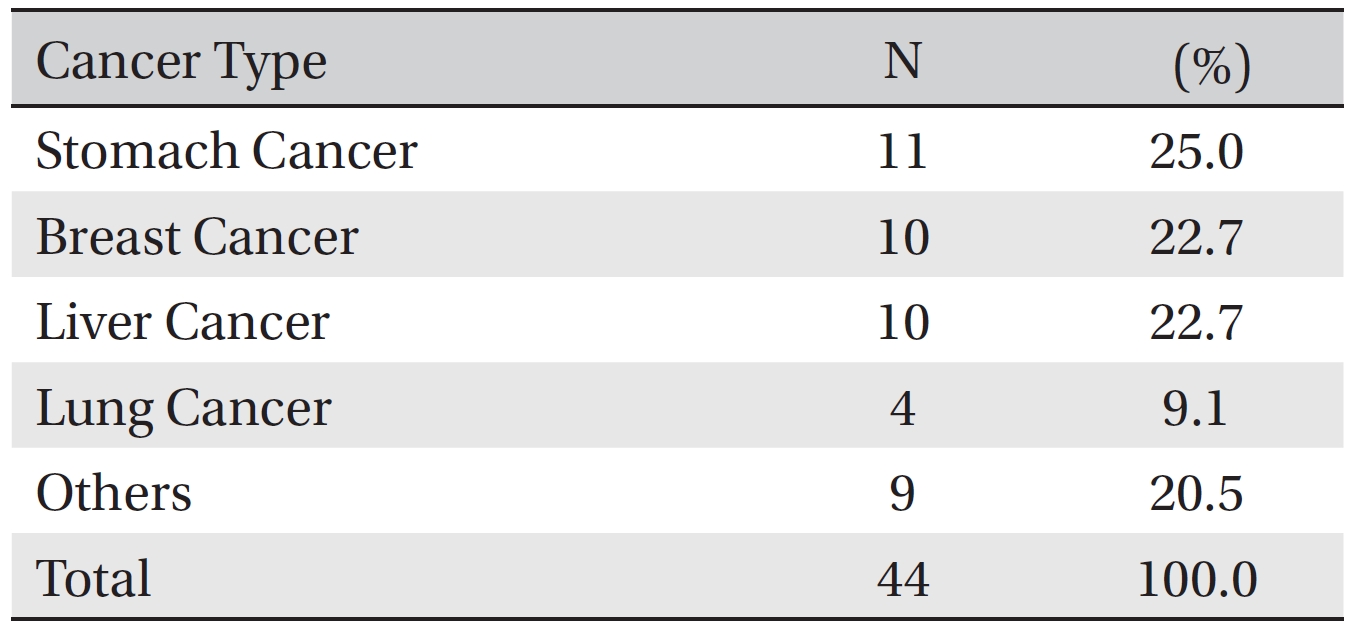
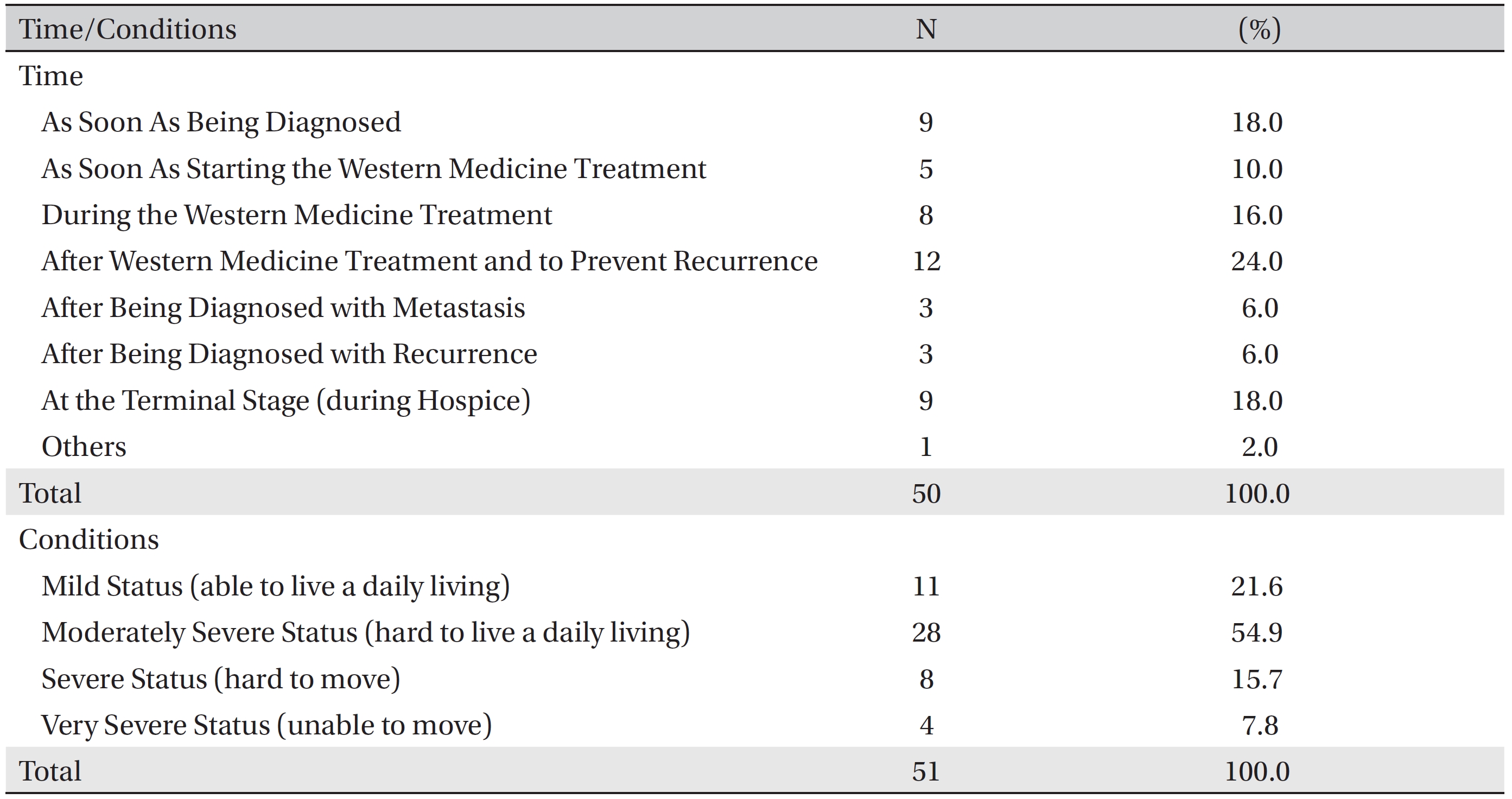
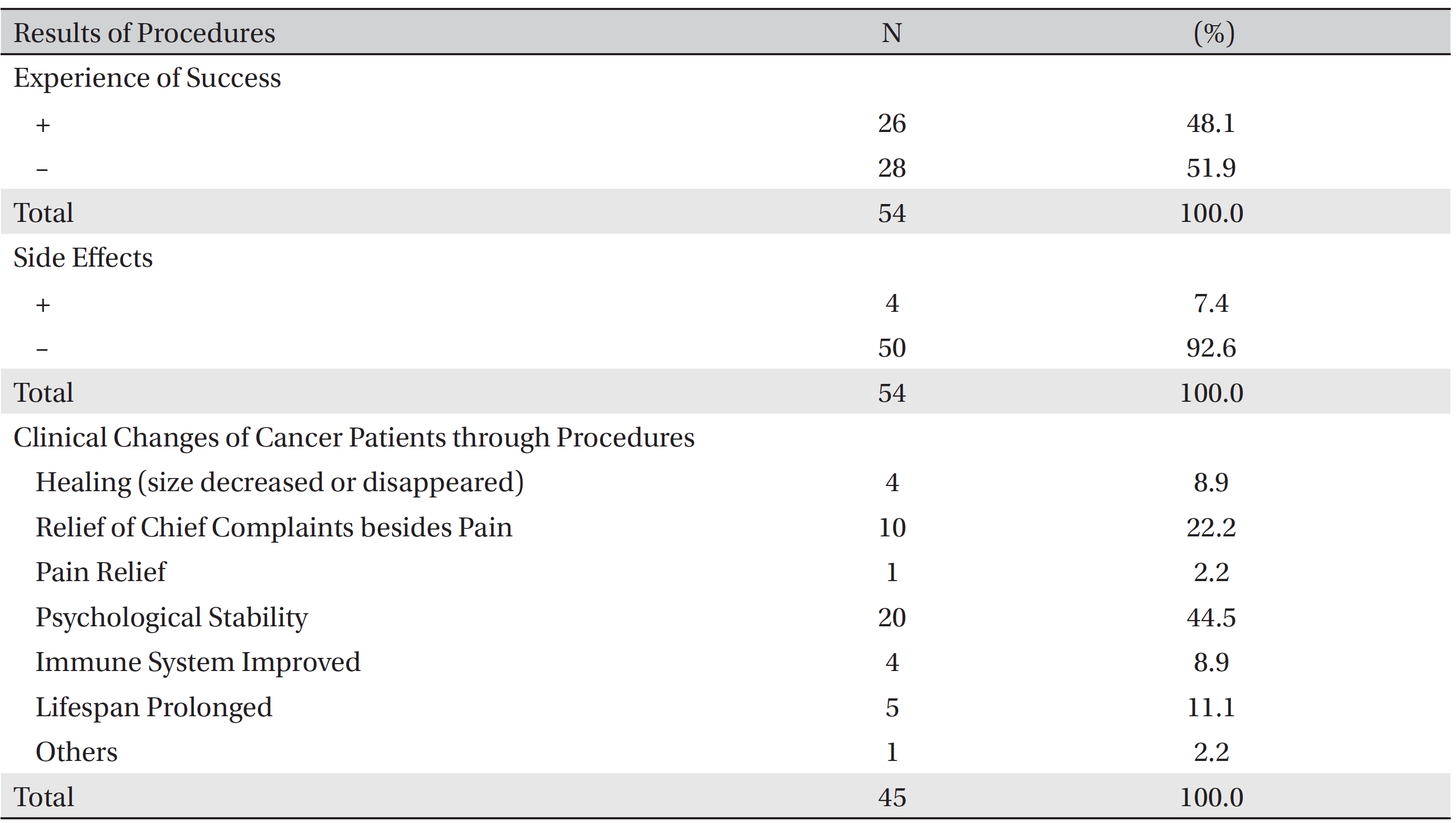
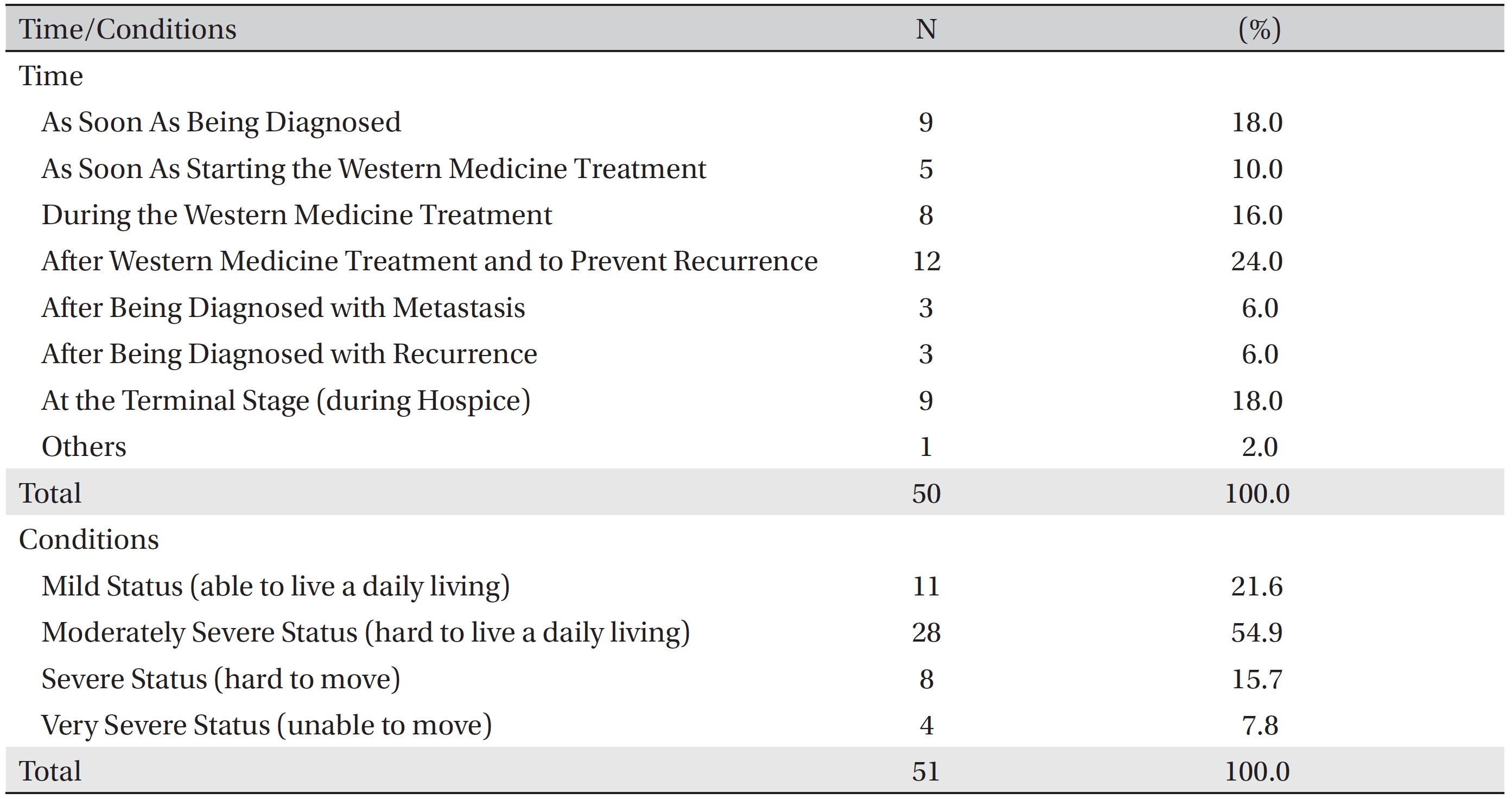
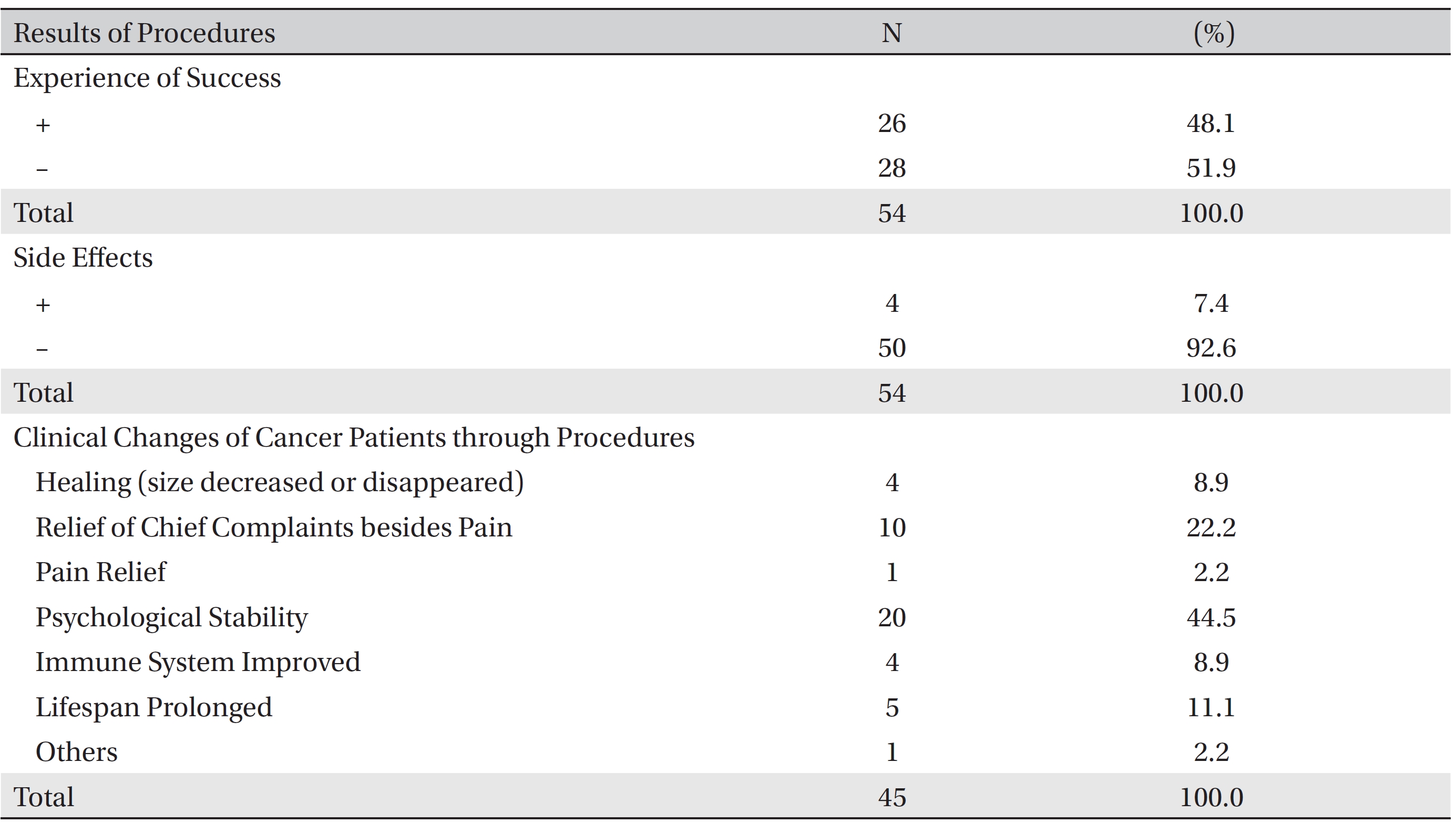
The kinds of cancers for which the patients received CAM procedures were stomach cancer (25.0%), breast cancer (22.7%) and liver cancer (22.7%) (Table 4) Cancer patients mostly received CAM after Western medicine treatment and to prevent recurrence (24.0%), at a terminal stage (18.0%), as soon as being diagnosed as having cancer (18.0%), and during Western medicine treatment (16.0%). In general, most patient (54.9%) started to receive CAM in a moderately severe stage of the cancer (Table 5) The rate of treating cancer patients with CAM was 48.1%, and side effects were encountered in 4 cases of CAM treatment (7.4%), with 2 of the 4 patients having been previously informed that CAM might have side effects. The effects of CAM on cancer patients were regarded mostly as psychological stability (44.5%) and relief of chief complaints besides pain (22.2%) (Table 6).
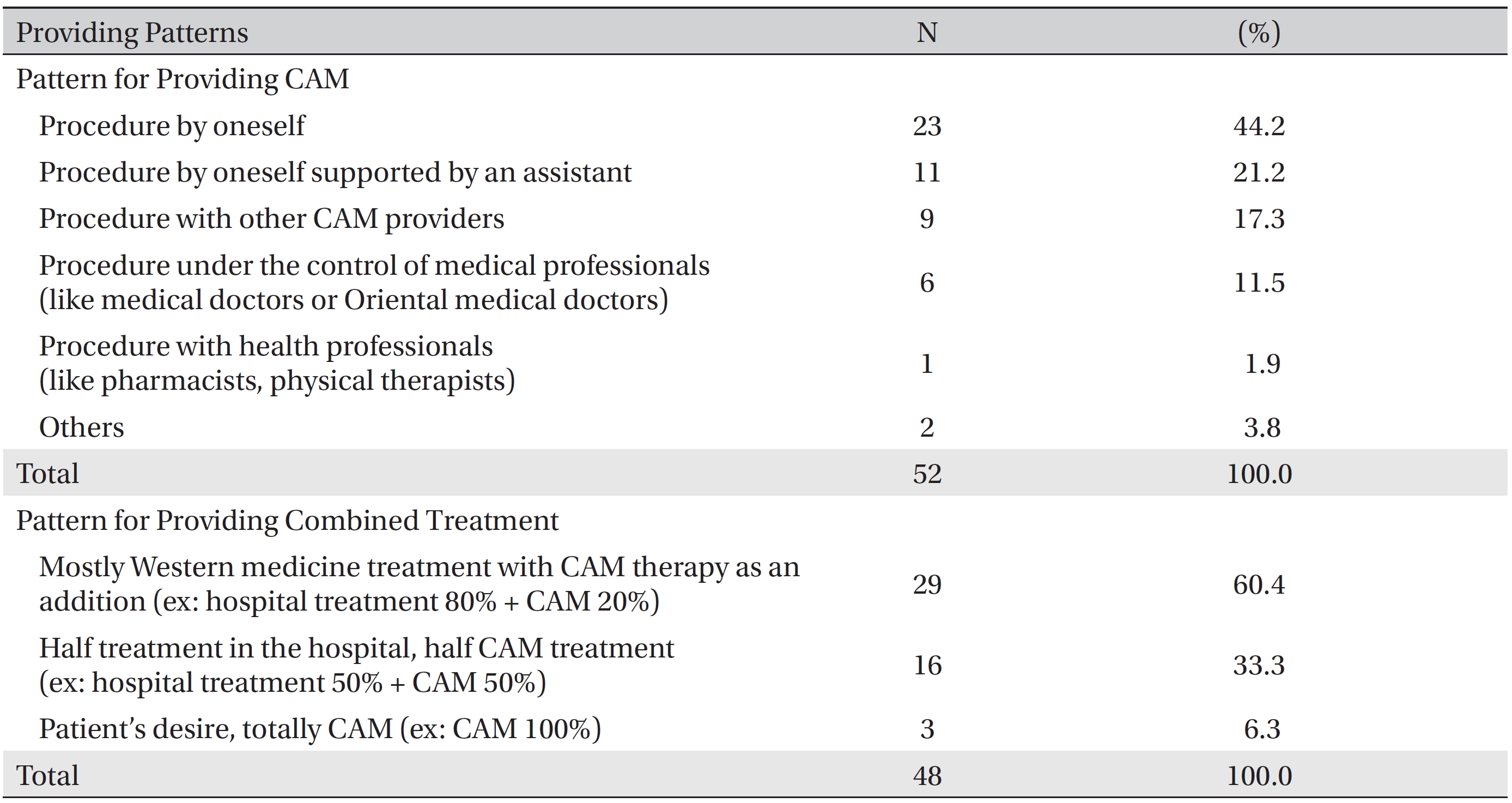
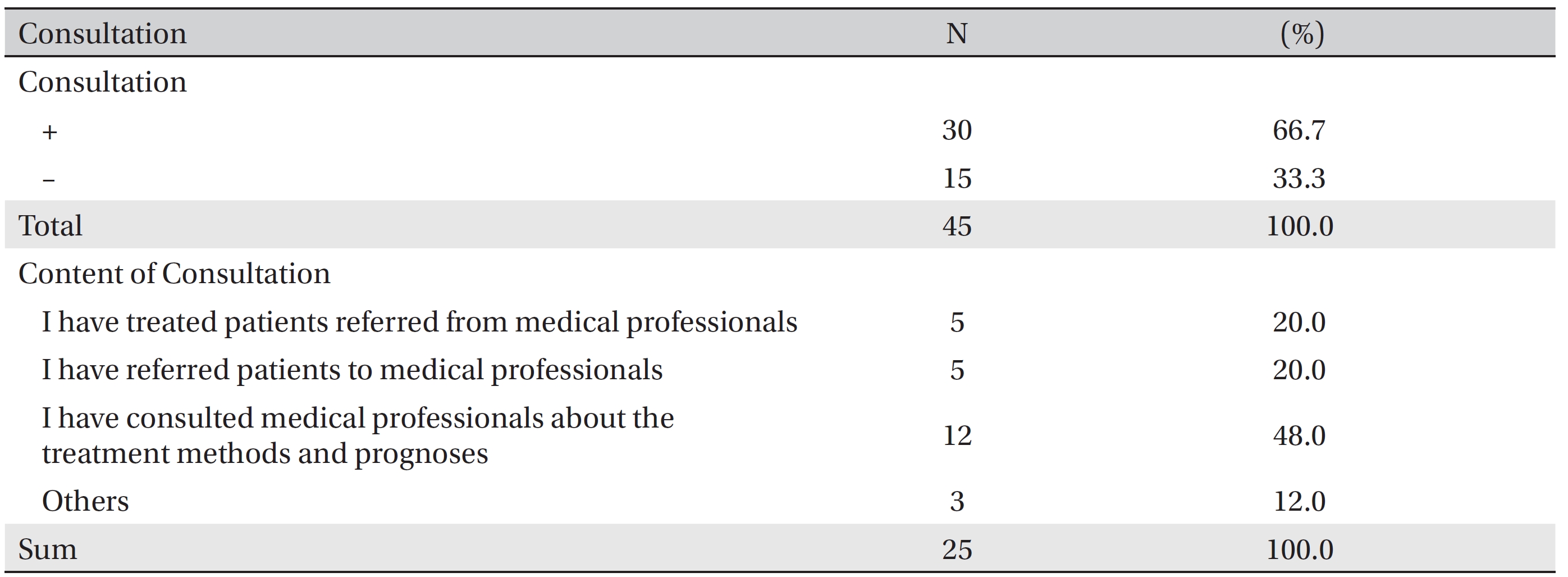
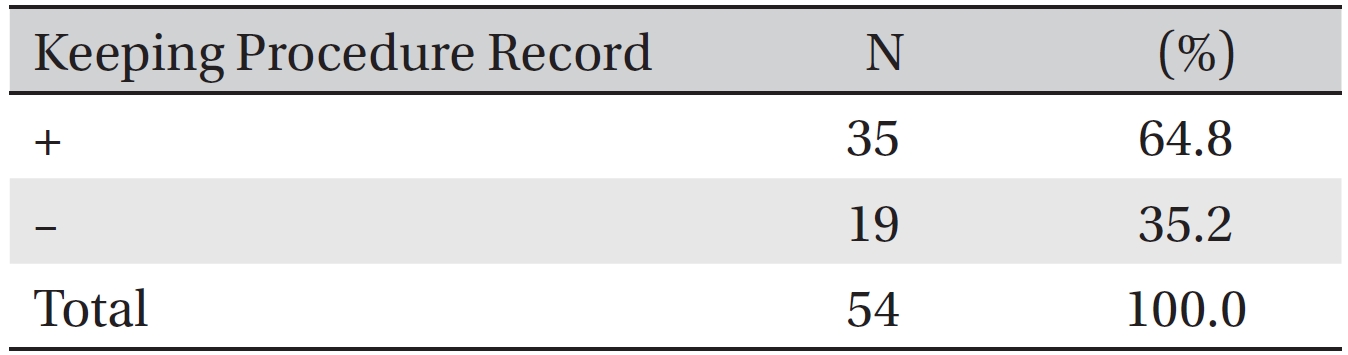
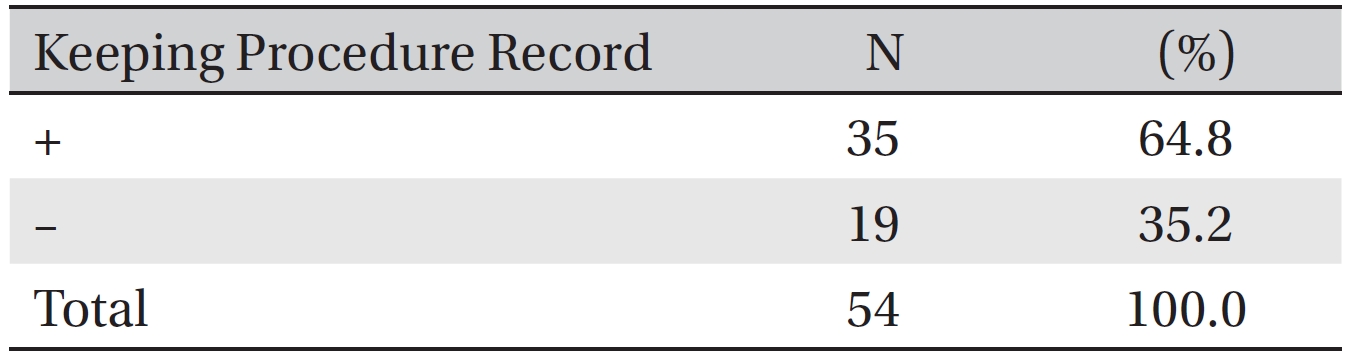
The pattern for providing CAM treatment to cancer patients was mostly a practitioner administrating CAM by himself/herself and/or a practitioner supported by an assistant (65.4%). As many as 50% to 80% of the cancer patients simultaneously received CAM and Western medicine treatment (Table 7) The rate of consultations with medical professionals was 66.7% (Table 8) Of the 54 surveyees providing data, 64.8% kept procedure records (Table 9). For medical professionals, 90.0% kept records, and for other CAM providers, the rate was 52.9%.
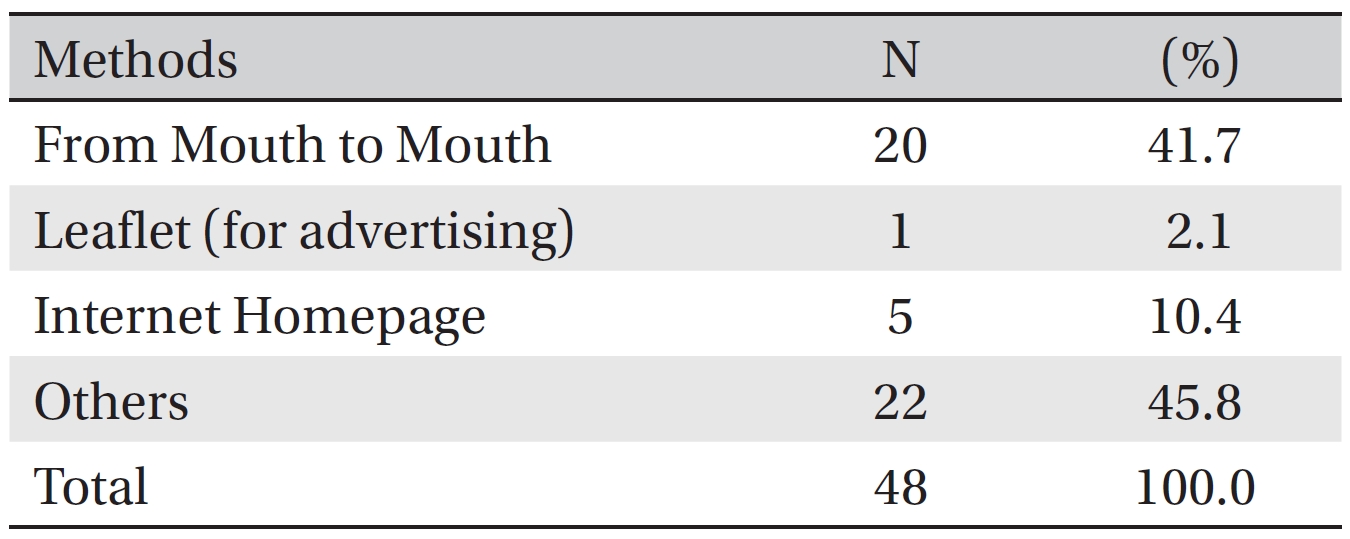
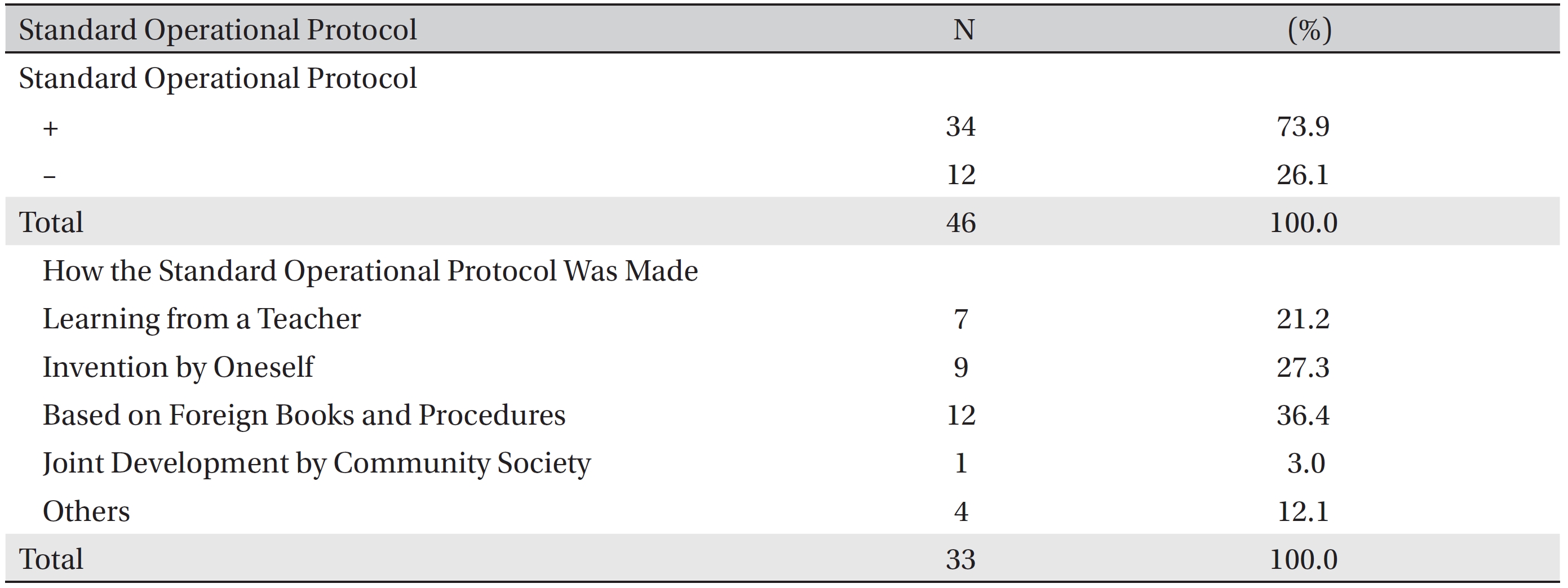
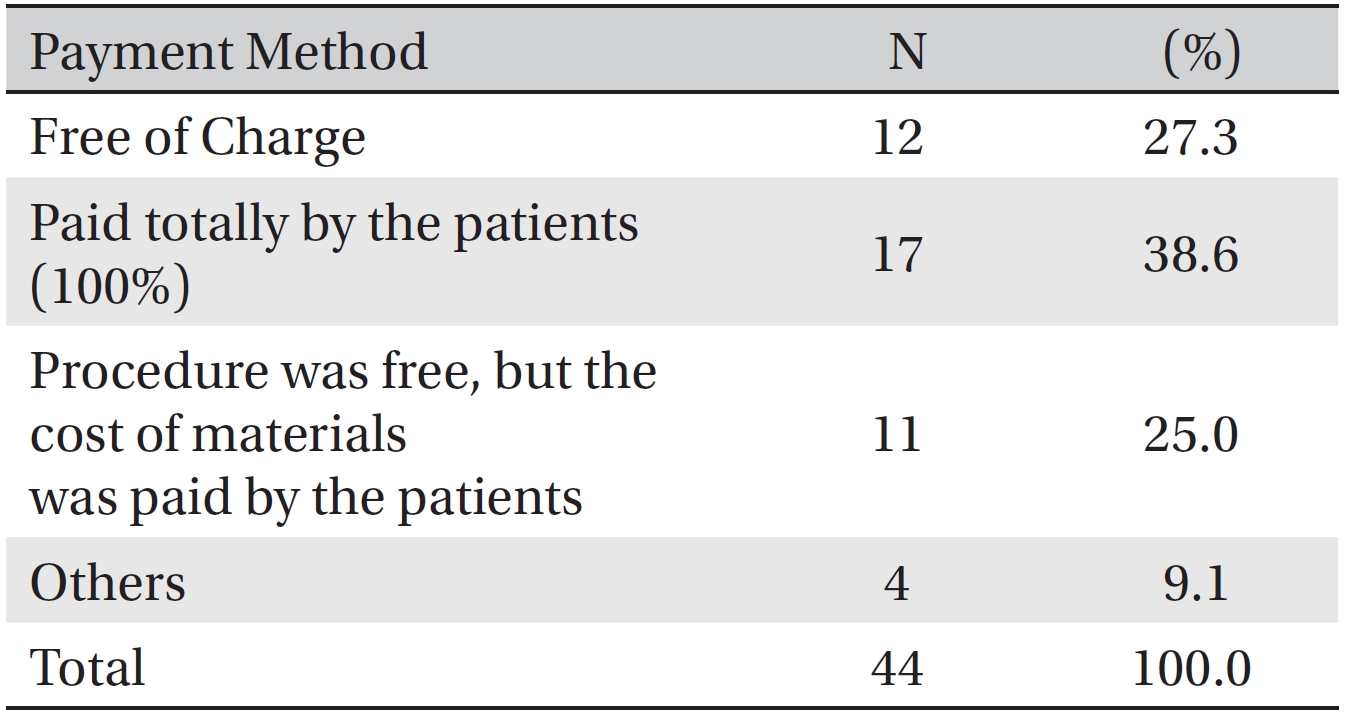
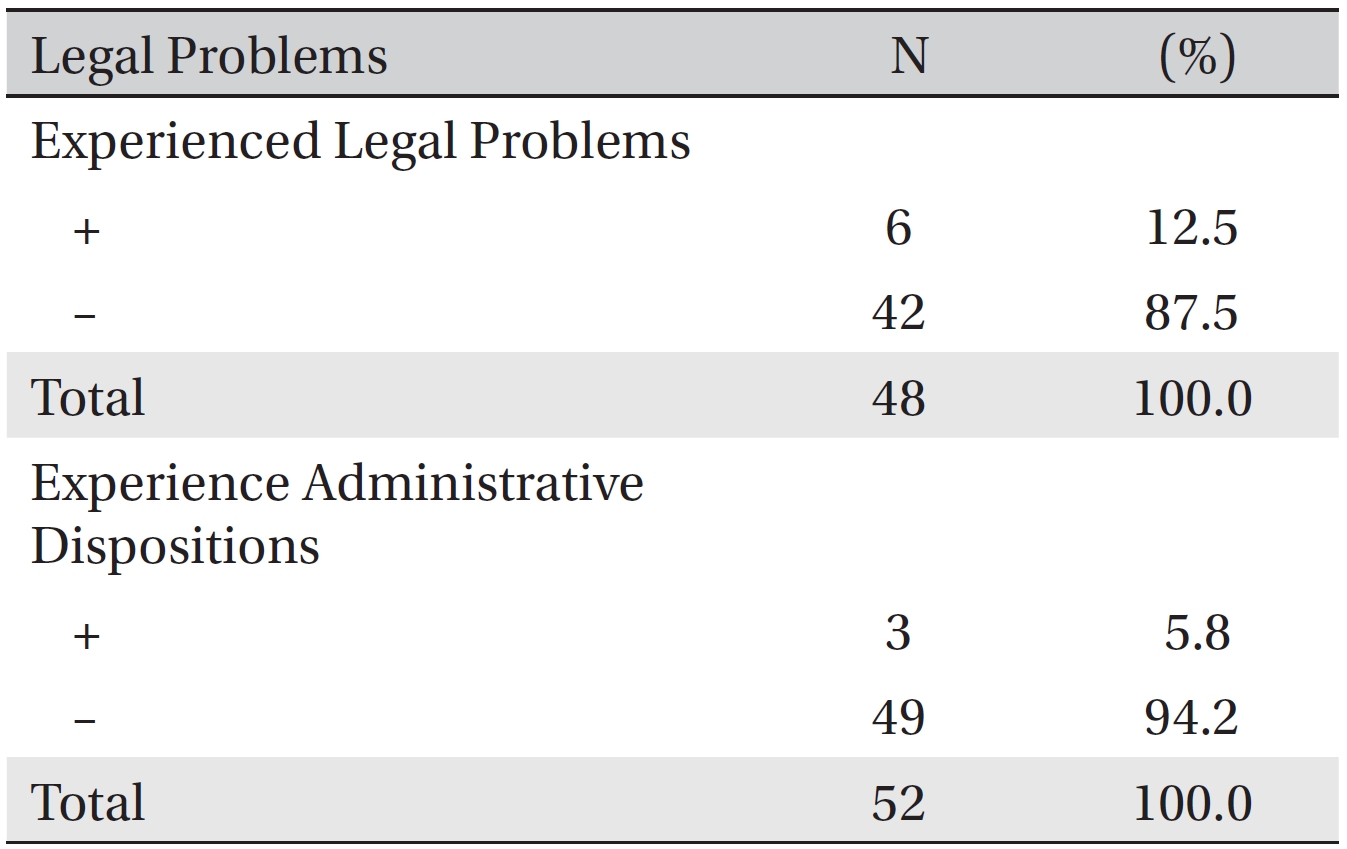
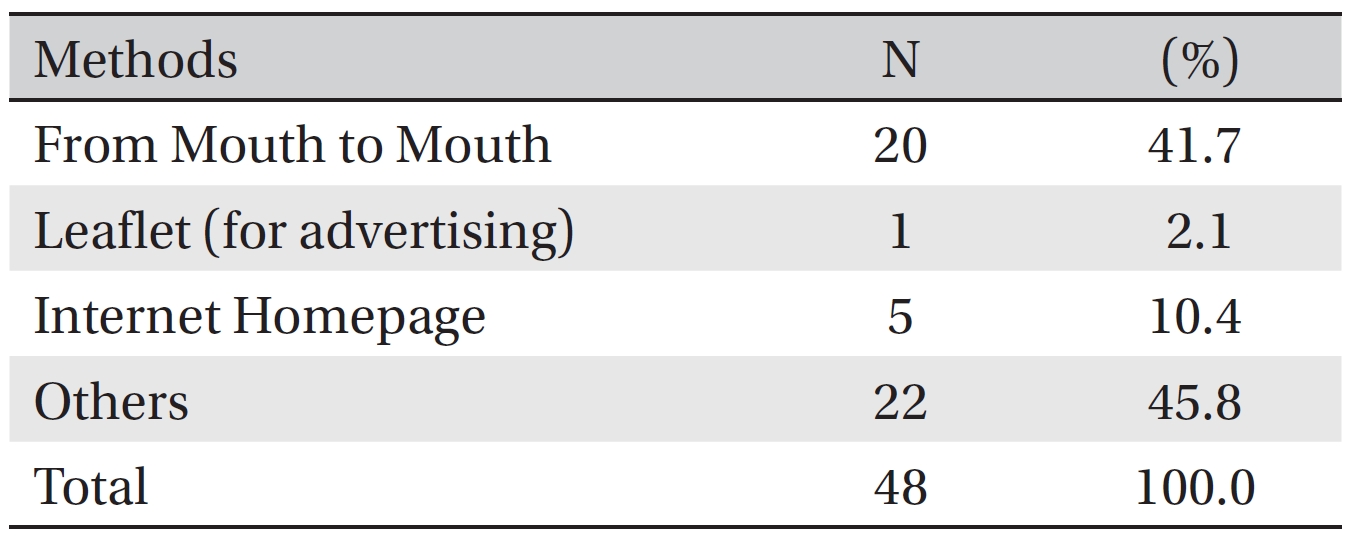
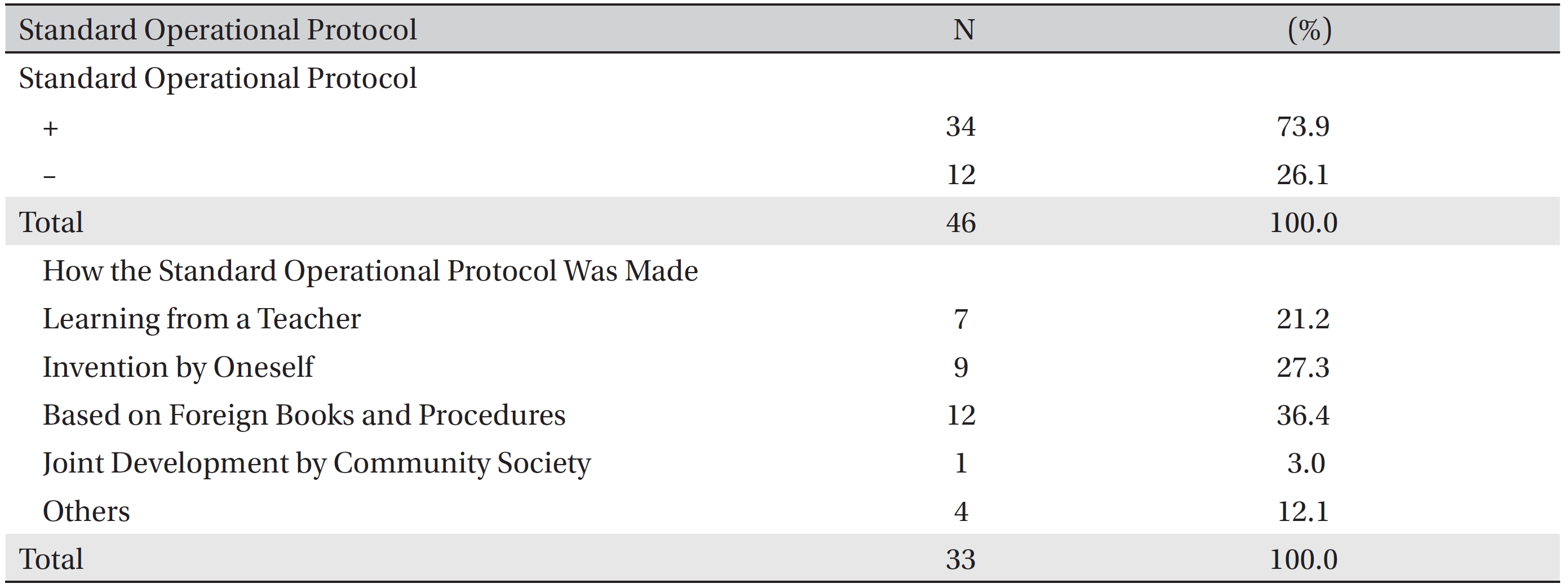
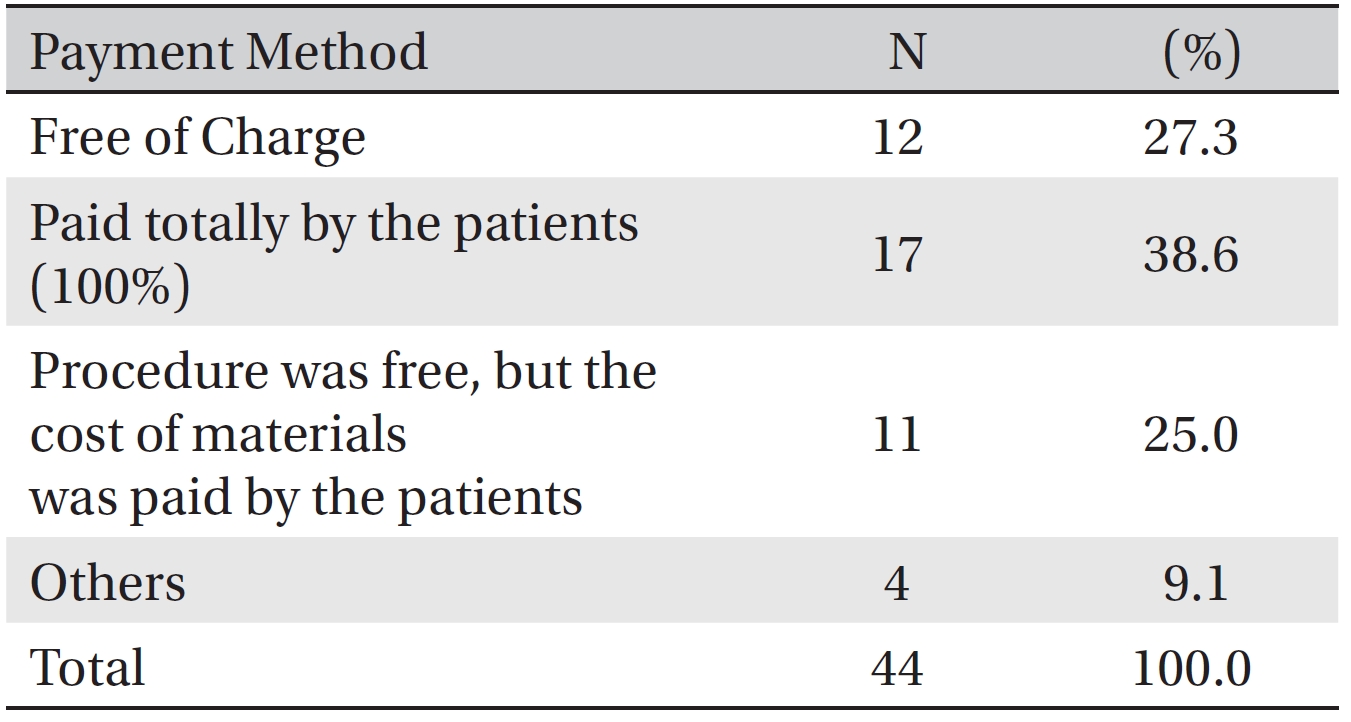
The advertising method for CAM was introduction by word of mouth (41.7%) and the internet (10.4%) (Table 10) Of the 46 surveyees providing data on the standard operational procedure for CAM, 73.9% (34/46) had such procedures, and those procedures were based on foreign books and procedures (12/33, 36.4%), learning from teachers (7/33, 21.2%), and individual inventions (9/33, 27.3%) (Table 11) As the payment method for the procedure, for 12 of 44 cases (27.3%), the procedure was provided free of charge, for 17 of 44 cases (38.6%), the payment was borne totally by the patient, and for 11 of 44 cases (25.0%), the procedure was free of charge, but the cost of materials was paid by the patient (Table 12) After CAM treatment had been provided, 6 of 48 patients (12.5%) experienced legal problems, and 3 of 52 (5.8%) were involved in administrative dispositions (Table 13).
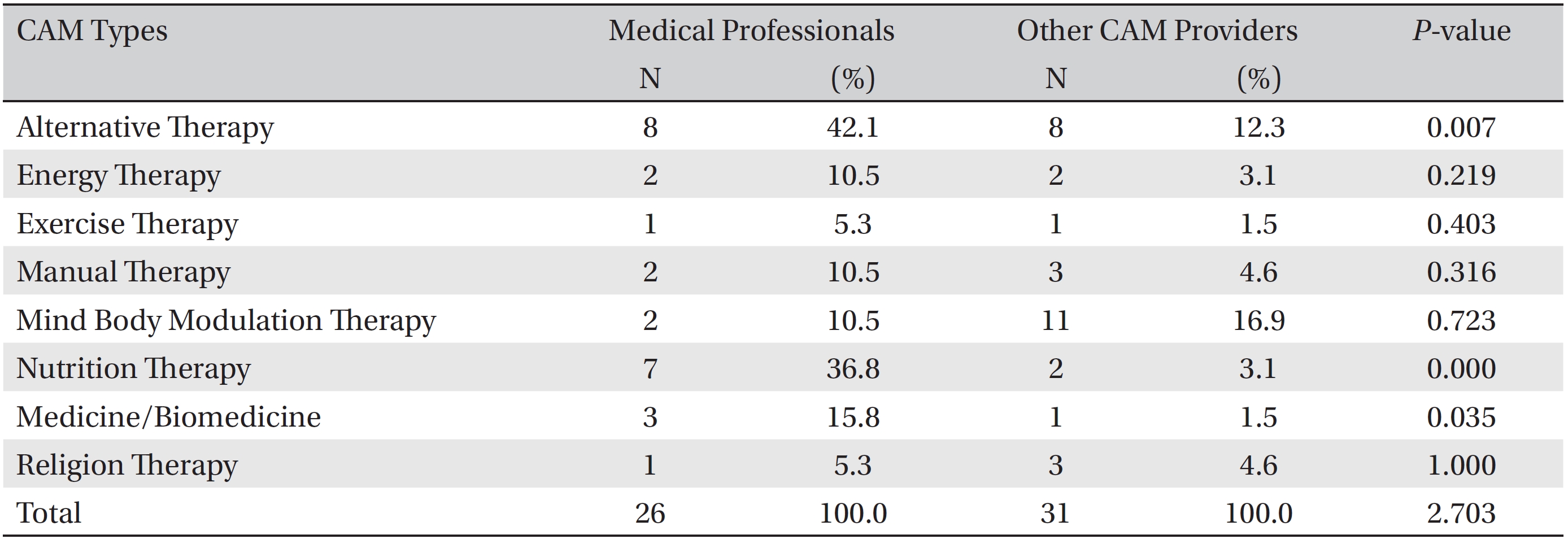
[Table. 3] CAM method as a procedure for cancer patients
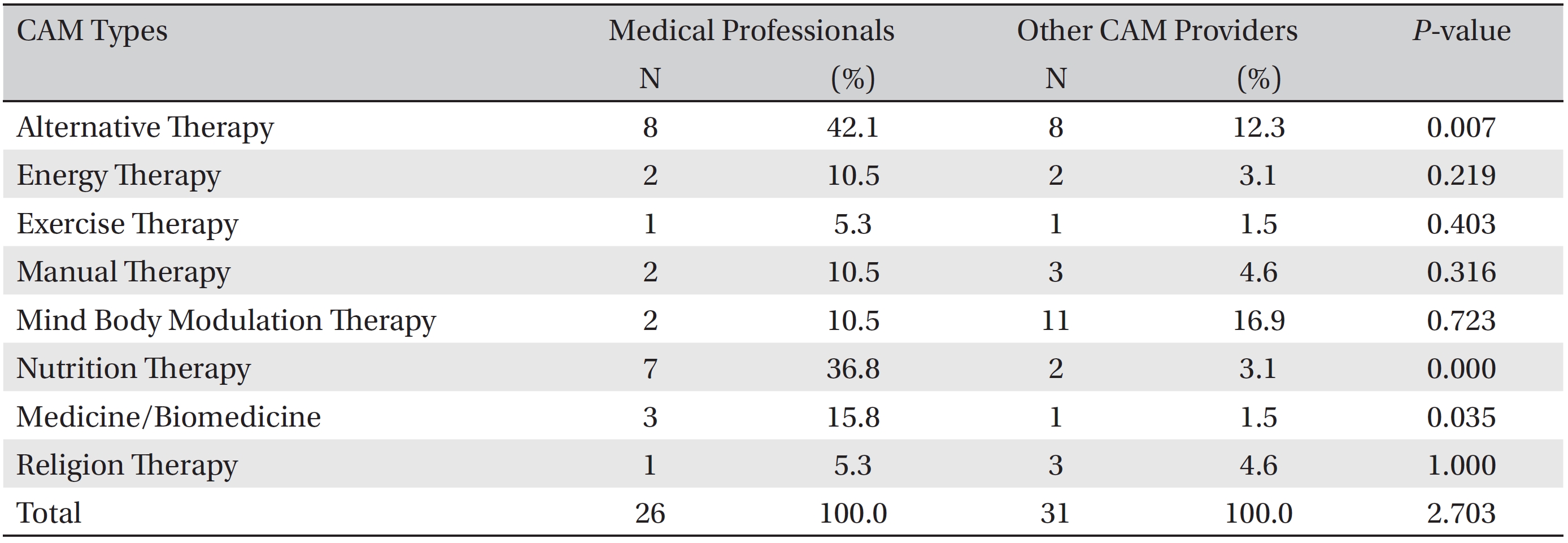
CAM method as a procedure for cancer patients
[Table. 4] Cancer types of the patients
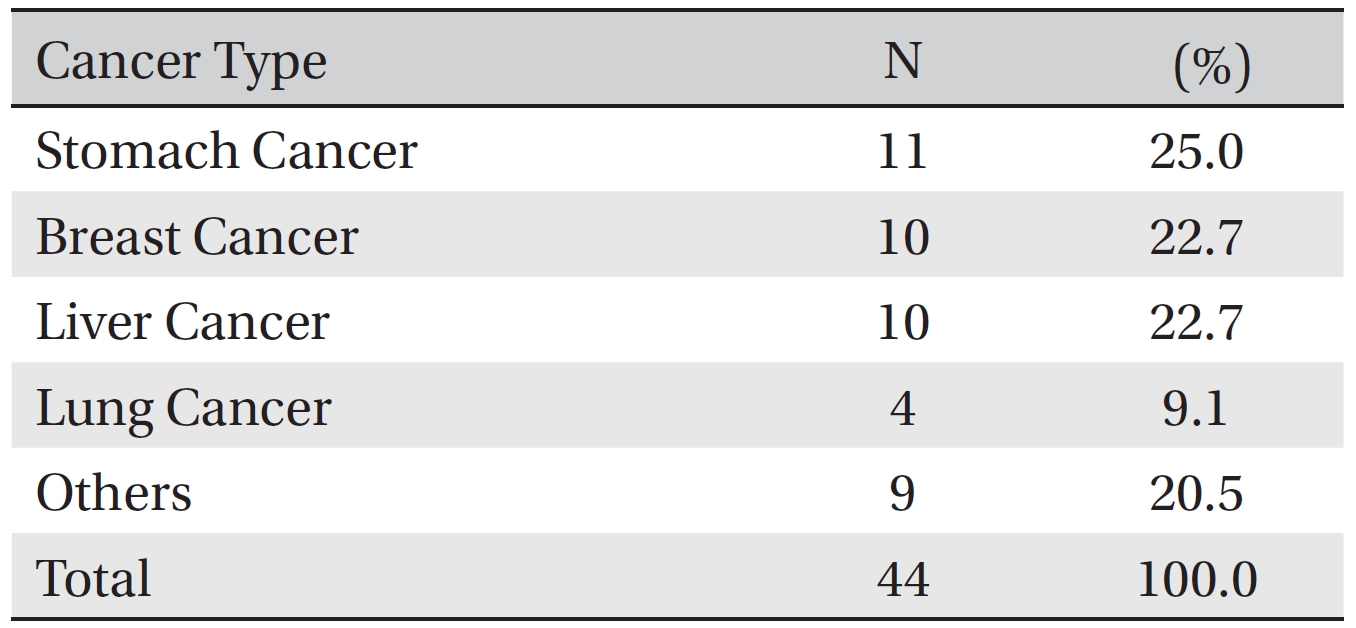
Cancer types of the patients
[Table. 5] Time when the cancer patients received CAM and their conditions
Time when the cancer patients received CAM and their conditions
[Table. 6] Results of procedures
Results of procedures
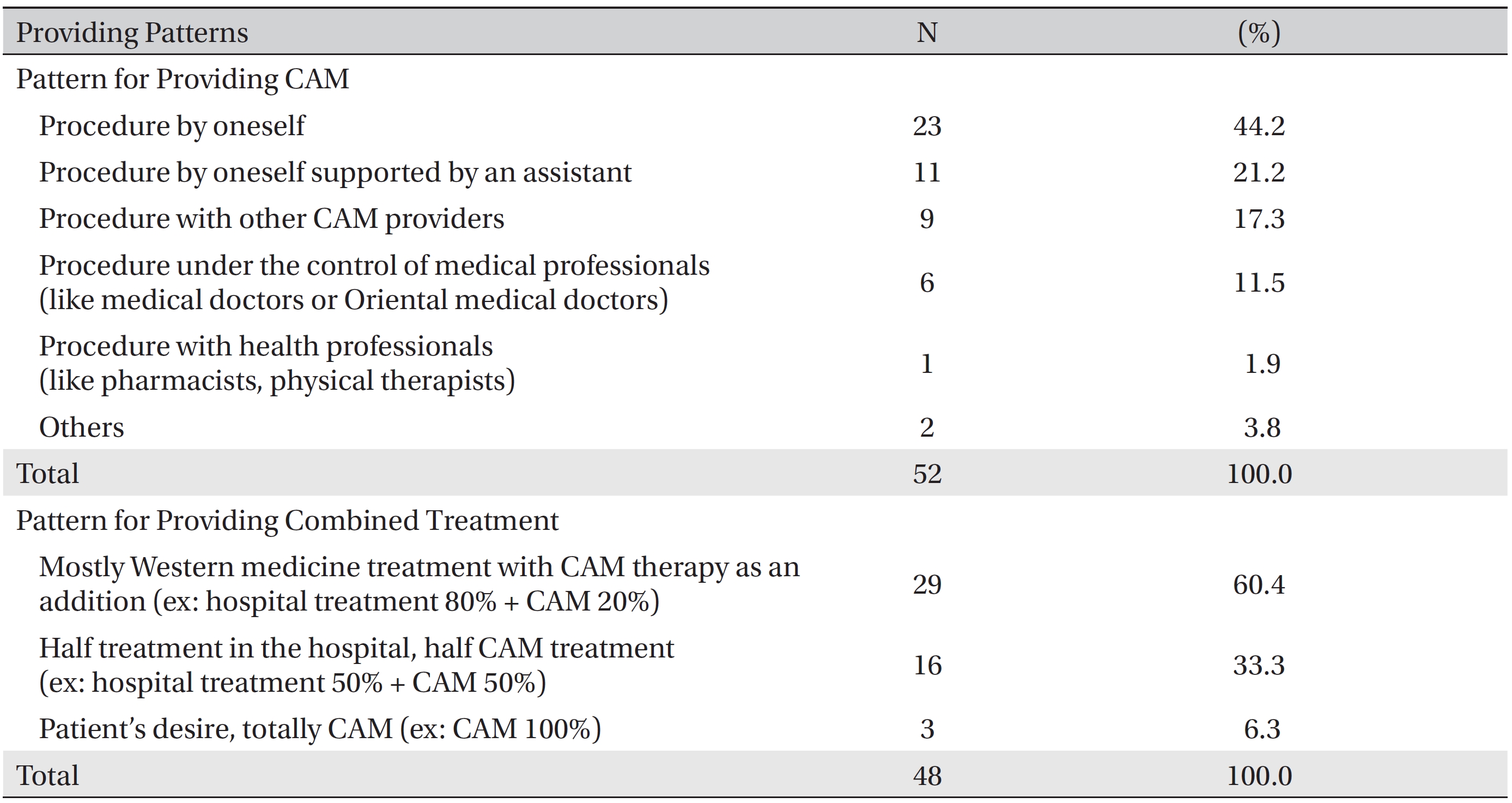
Pattern for providing CAM to cancer patients and for providing CAM combined with Western medicine treatment
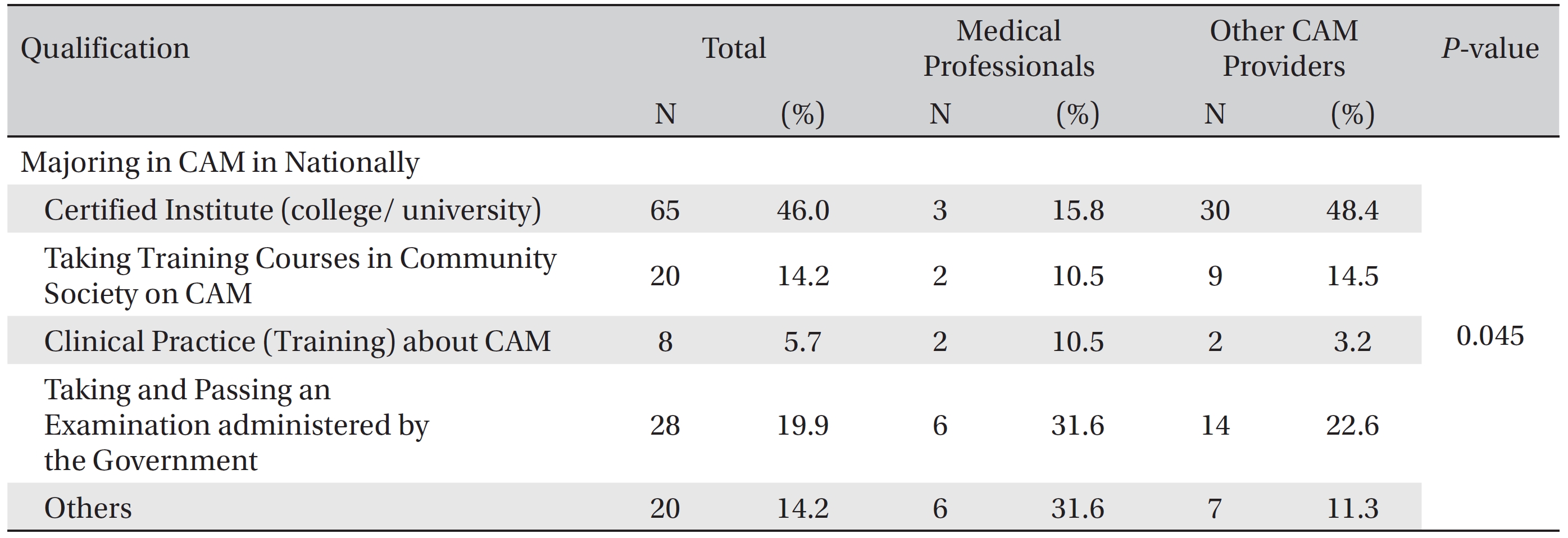
Of those surveyed, 65 out of 141 (46.1%) answered that CAM providers should take a CAM course at an institute (including college or university), 28 out of 141 (19.9%) answered that CAM providers should take and pass an examination administered by the government, and 20 out of 141 (14.2%) answered that CAM providers should take a training course given by a national special community society 14.2% (Table 14) Medical professionals (medical doctors/ oriental medical doctors/nurses) answered that taking and passing the examination was the most important factor (6/19, 31.6%). On the contrary, other CAM providers answered that education concerning CAM at an institute was more important than taking and passing an examination (
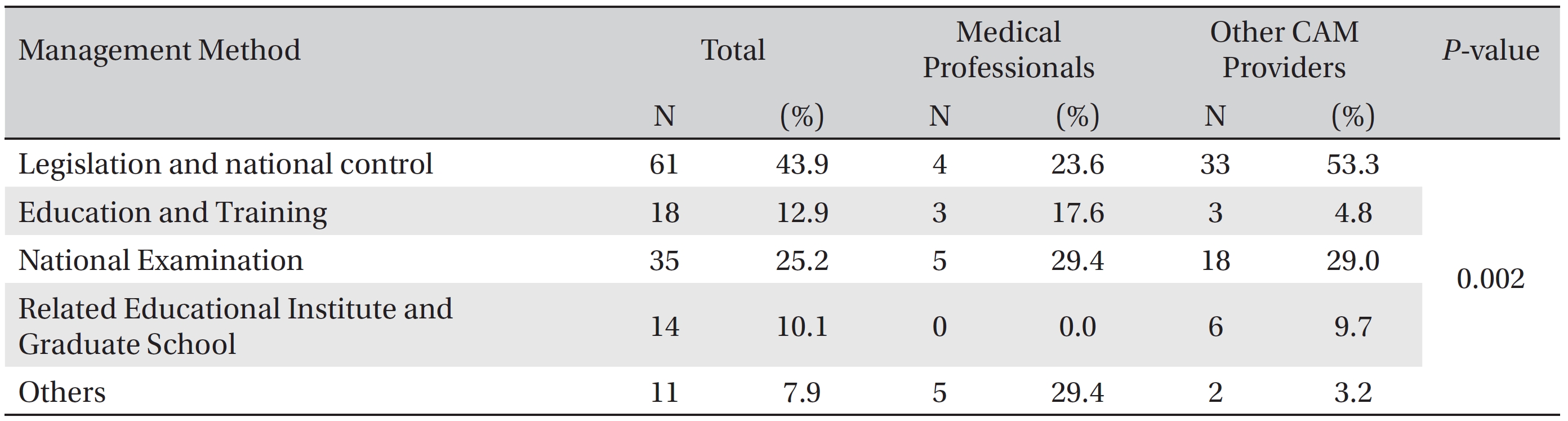
For the qualification method, 61 of the 139 (43.9%) surveyees providing such data answered that legislation and quality control by the national government to manage the quality control of CAM providers were preferred, and 35 of the 139 (25.2%) preferred a national examination for quality control (Table 15) Medical professionals were almost equally split among the options for quality control except for related education at an Institute or Graduate school, which received no support. However, CAM providers mostly wanted legislation and national management (33/62, 53.3%) and a national examination (18/62, 29.0%) (
[Table. 8] Consultation with medical professionals
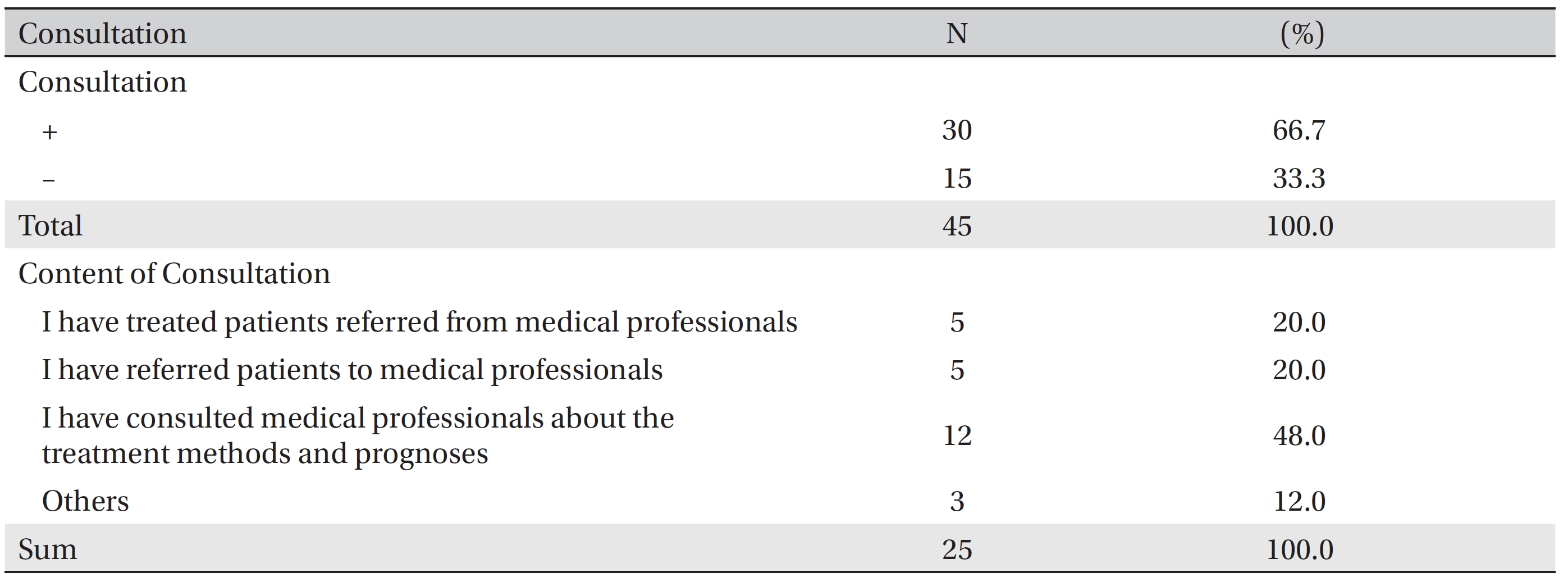
Consultation with medical professionals
[Table. 9] Keeping a procedure record
Keeping a procedure record
[Table. 10] Advertising method
Advertising method
[Table. 11] Standard operational procedure or protocol for CAM
Standard operational procedure or protocol for CAM
Western medicine and CAM, including home remedies, are mainly used in Europe and America; thus, if one considers how to control and manage that system, one must think about which CAM remedies and/or treatments are effective and beneficial. Korea, on the contrary, has three kinds of medical systems: Oriental medicine, Western medicine, and CAM, including home remedies; thus, Korea’s situation is somewhat confusing and difficult to manage. Koreans especially tend to depend on many home remedies and medicines. Culturally, Koreans buy food and supplements based on word of mouth from neighbors, so they are apt to select CAM treatments, and the utilization rate of CAM is very high.
[Table. 12] Methods for payment of the procedure fee for patients treated with CAM
Methods for payment of the procedure fee for patients treated with CAM
[Table. 13] Legal problems for patients treated with CAM (medical disputes included)
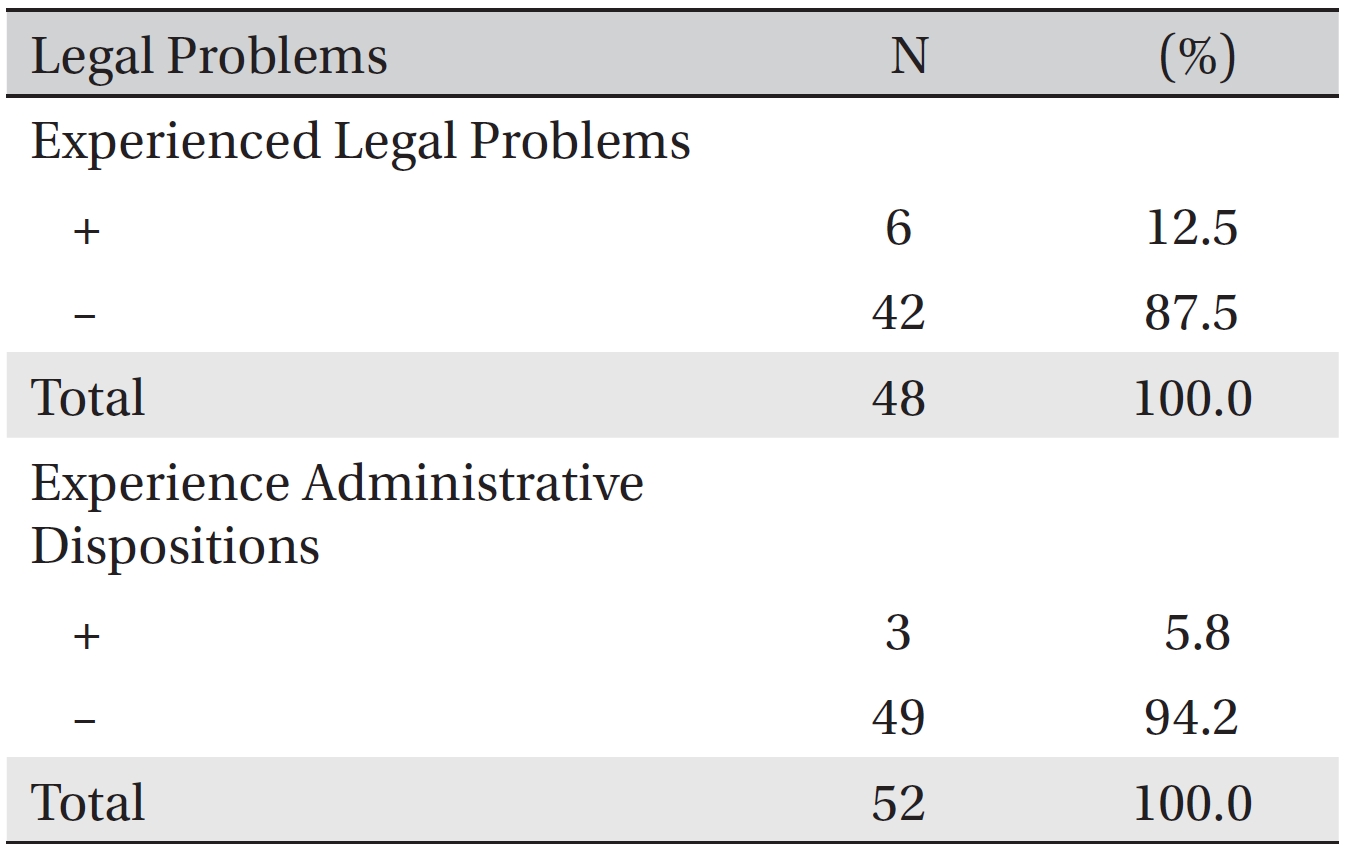
Legal problems for patients treated with CAM (medical disputes included)
[Table. 14] Opinions on qualification method for CAM providers
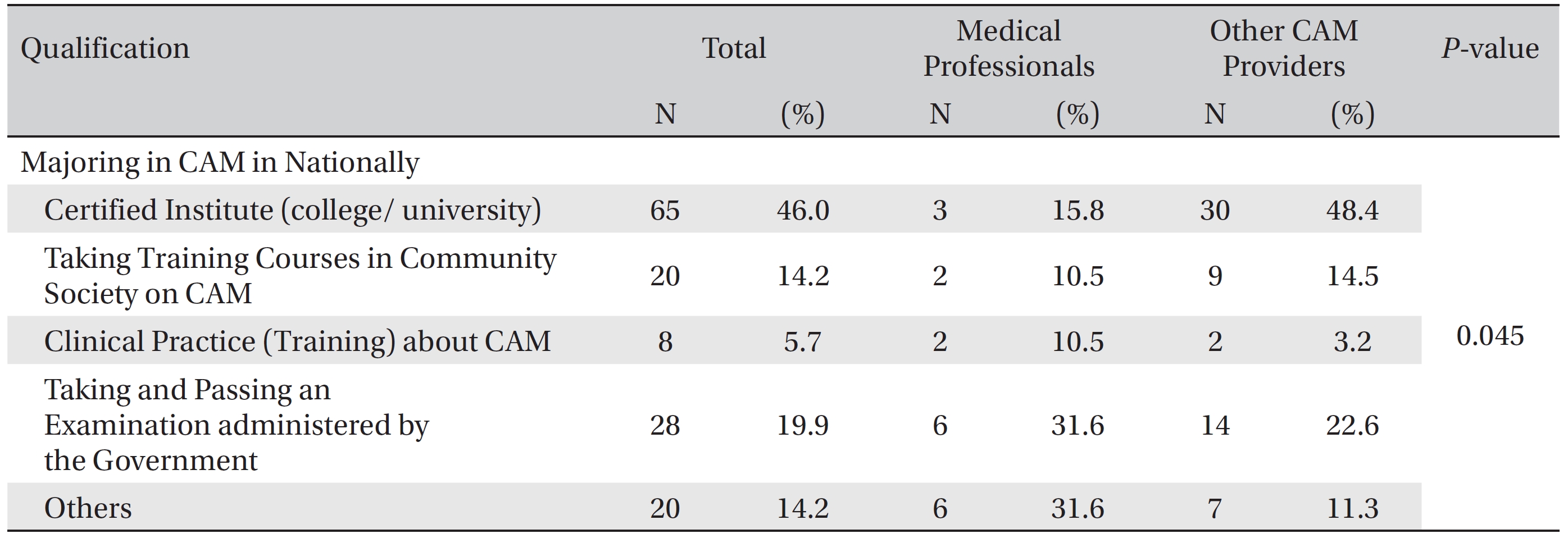
Opinions on qualification method for CAM providers
The reasons we consider this problem and the need for a new policy on CAM providers are as follows: First, medical expenditure is growing in Korea, as well as in the United States, so control policies should cut medical expenditures. Second, Korea’s medical policy only focuses on the national health insurance system. Third, the growing economic power of the CAM market will allow more diversity in terms of health information, products and services. Fourth, Western medicine treatments are mostly refunded by the national health insurance system, so the treatment fee is strictly controlled. On the other hand, CAM practitioners, who are not be reimbursed by the national health insurance system, can make money arbitrarily. Fifth, Western medicine was developed based on modern science and research and does not usually consider the connection between the body and the mind. Sixth, among CAM, Oriental medicine and home remedies in Korea are rooted almost in the same tradition and culture (cultural and emotional band). Seventh, there is a problem concerning the health information on CAM reported in mass media and whether it is trustworthy or not. Eighth, modern Western treatments are very severe and have side effects, so people who want to receive safer and non-invasive treatments with as few side effects as possible seek CAM. Ninth, few data on the side effects of CAM treatments exists, so consumers are easily led to believe CAM treatments have no side effects, so CAM providers are usually not subjected to lawsuits.
The government should pay attention to the differences between CAM and Oriental medicine that can lead to many invasive treatments [9]. The government should intervene and actively manage CAM and Oriental medicine. On the other hand, as another method of management, CAM, which is related to supplements with few side effects, could be self-regulated. But, if CAM related supplements have toxic effects or many side effects, then attention must be given to those supplements, and guidelines must be made in cooperation with the Korea Food and Drug Administration (KFDA), the Association of Korean Oriental Medicine (AKOM) and the Korean Medical Association (KMA). Analyzing these questionnaires, we found that many surveyees wanted a governmental regulation and management system for CAM providers.
[Table. 15] Opinions on qualification method for CAM providers
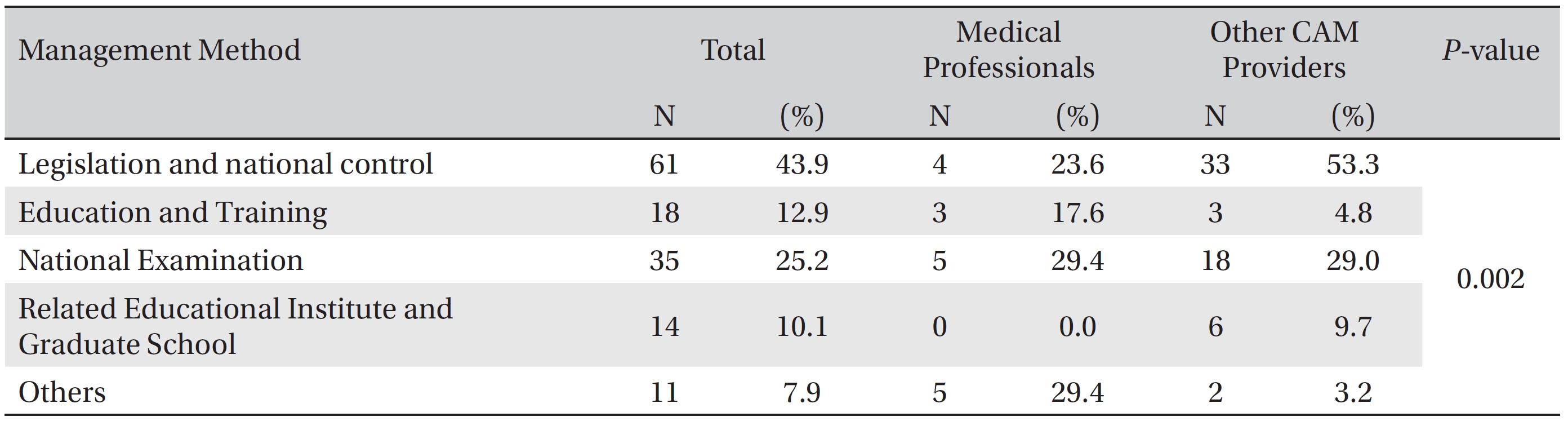
Opinions on qualification method for CAM providers
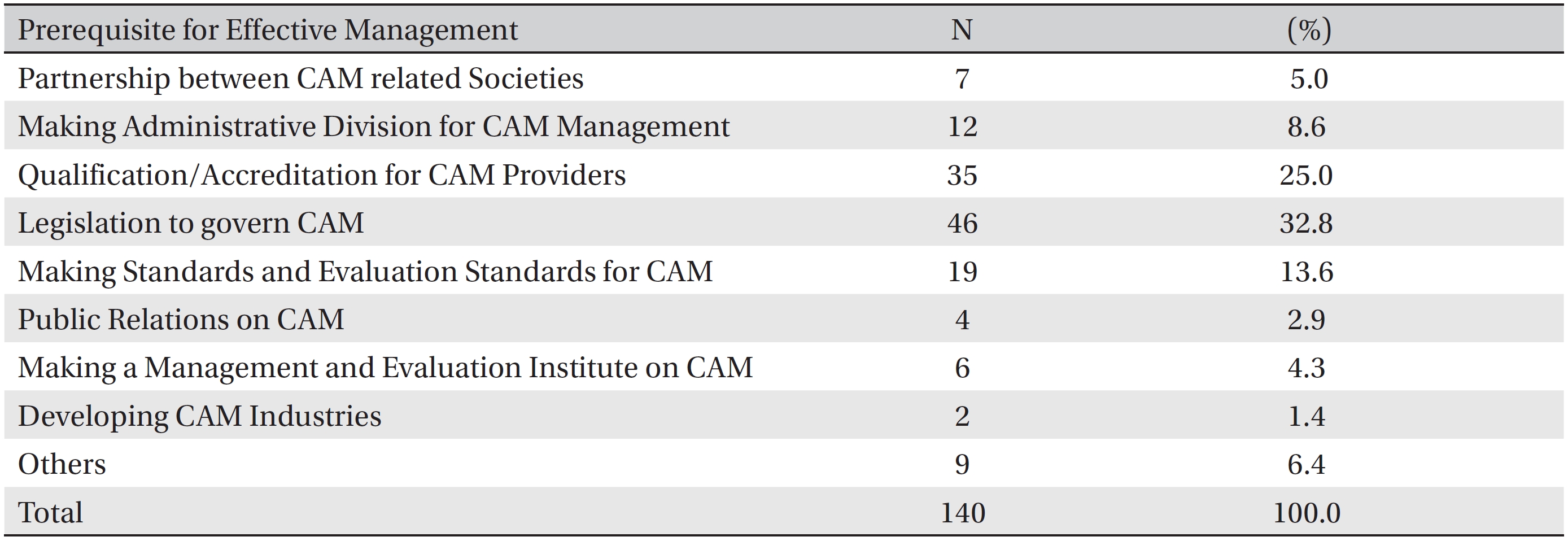
[Table. 16] Prerequisite for effective management of CAM providers
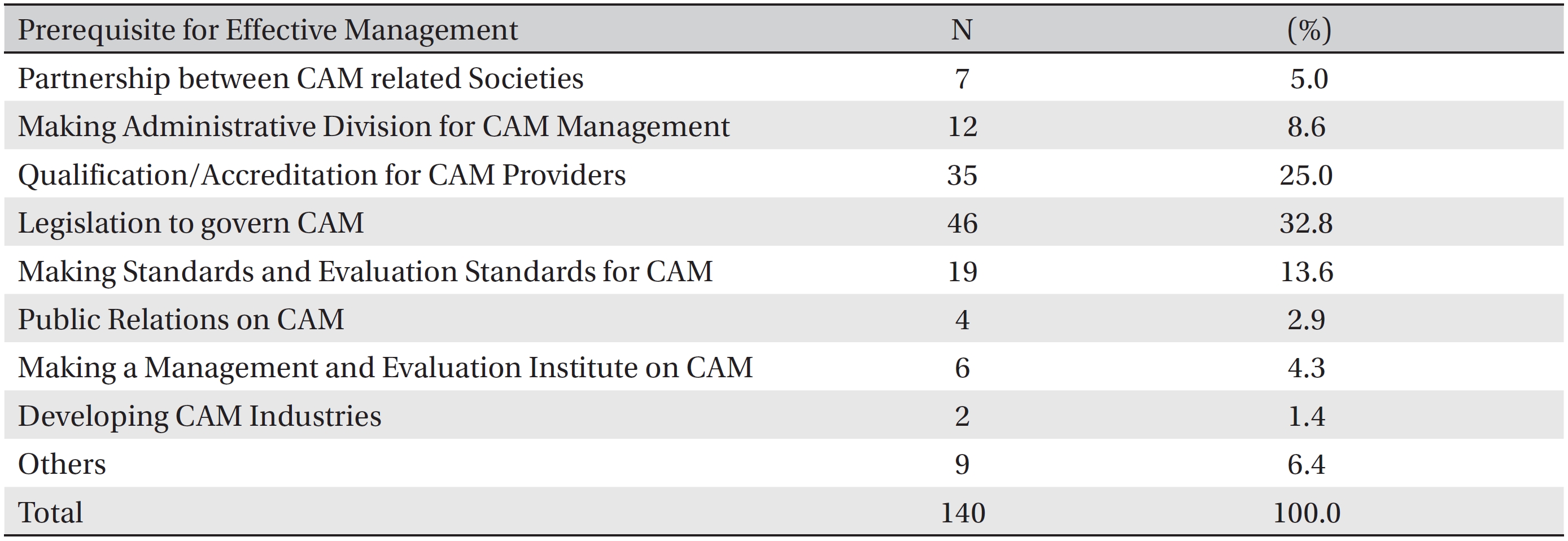
Prerequisite for effective management of CAM providers
In terms of a medical social study, the need for CAM is increasing with the help of mass media and the internet because CAM can make up for the shortcomings of Western medicine and CAM can help people who want to treat their diseases and maintain their health. Thus, in Korea, an administrative department to govern CAM and develop CAM policy to help promote health should be established, and that department should have a long-term, concise plan like the National Center of Complementary and Alternative Medicine (NCCAM) in America does.
When cancer patients use CAM, the patients prefer nutritional methods like food, supplements, and herb medicine. On the contrary, CAM providers prefer alternative therapy, mind body intervention therapy, and nutritional therapy. Procedures for treating cancer patients existed more often with medical professionals than with other CAM providers, and the medical professionals kept better medical records. Medical professionals very often used alternative therapy, nutritional therapy, and medicine/ biotherapy. Side effects were very few, only 4 cases in this study (7.4%). Legal problems and administrative dispositions were encountered in 12.5% and 5.8%, respectively, of the cases. In terms of qualification or quality control, medical professionals and other CAM providers have different viewpoints. For example, some CAM providers claimed that both legislation and official education on CAM or a national examination is needed as a first step; then, a license test is needed for quality control. To the contrary, medical professionals claimed that a license test is needed as a first step, followed by legislation.